
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






Last week, I accompanied my sister-in-law for a prenatal checkup and ran into an acquaintance in the hallway—she was 32 weeks pregnant and her water had broken suddenly.
The nurse rushed her to the delivery room, and the mother only had time to say: “It’s only 32 weeks, why did my water break?”

The baby was born that day and was immediately admitted to the neonatal intensive care unit.
My sister-in-law clutched my hand and asked: “All her prenatal checkups were normal, so why did she go into preterm labor?”
I opened my mouth but couldn’t say a word.
——How could a baby be born prematurely even when the mother had all normal checkups and took folic acid every day?
I later asked several doctors about this case, and all gave similar answers.
Preterm birth has no single cause.
Even common inflammation, infection, or problems with the cervix and placenta can trigger preterm labor.
Complications during pregnancy, combined with irregular daily routines or improper nutrition, can all act as triggers for preterm birth.
I frowned.
After returning home, I repeatedly searched keywords: preterm birth, folate, cord blood, and gestational age.
At first, the information I found was the usual advice: take folate when trying to conceive and in early pregnancy, mainly to prevent neural tube defects.
It wasn’t until I came across a 2023 study that I noticed a previously overlooked indicator—5-methyltetrahydrofolate, also known as 5-MTHF, the active form of folate.
This study was published in the *European Journal of Clinical Nutrition* as a large-sample paper.
Researchers measured 5-MTHF levels in cord blood of 124 newborns and compared them with thiamine diphosphate data to explore links between these nutritional metabolic markers, preterm birth, and fetal development.
Among the 124 infants:
- 26 were early preterm infants born before 32 weeks
- 38 were late preterm infants born between 32 and 37 weeks
- 60 were full-term infants as controls
This grouping was designed to examine whether folate status differed in infants born earlier.
Several notable findings emerged.
What caught my attention was that late preterm infants (32–37 weeks) also had significantly lower 5-MTHF levels in cord blood.
This difference was unrelated to singleton or multiple pregnancies.
Fetal active folate status in utero varies inherently.
Thiamine diphosphate levels also changed: overall higher in preterm infants, but lower in multiples than singletons.
However, no clear association was found between thiamine diphosphate and small-for-gestational-age (SGA) infants.
The key finding for pregnant women in this study is 5-MTHF.
After multivariate analysis, the conclusion was clear:
Higher 5-MTHF levels in cord blood were associated with longer gestational age, higher birth weight, and longer body length at birth.
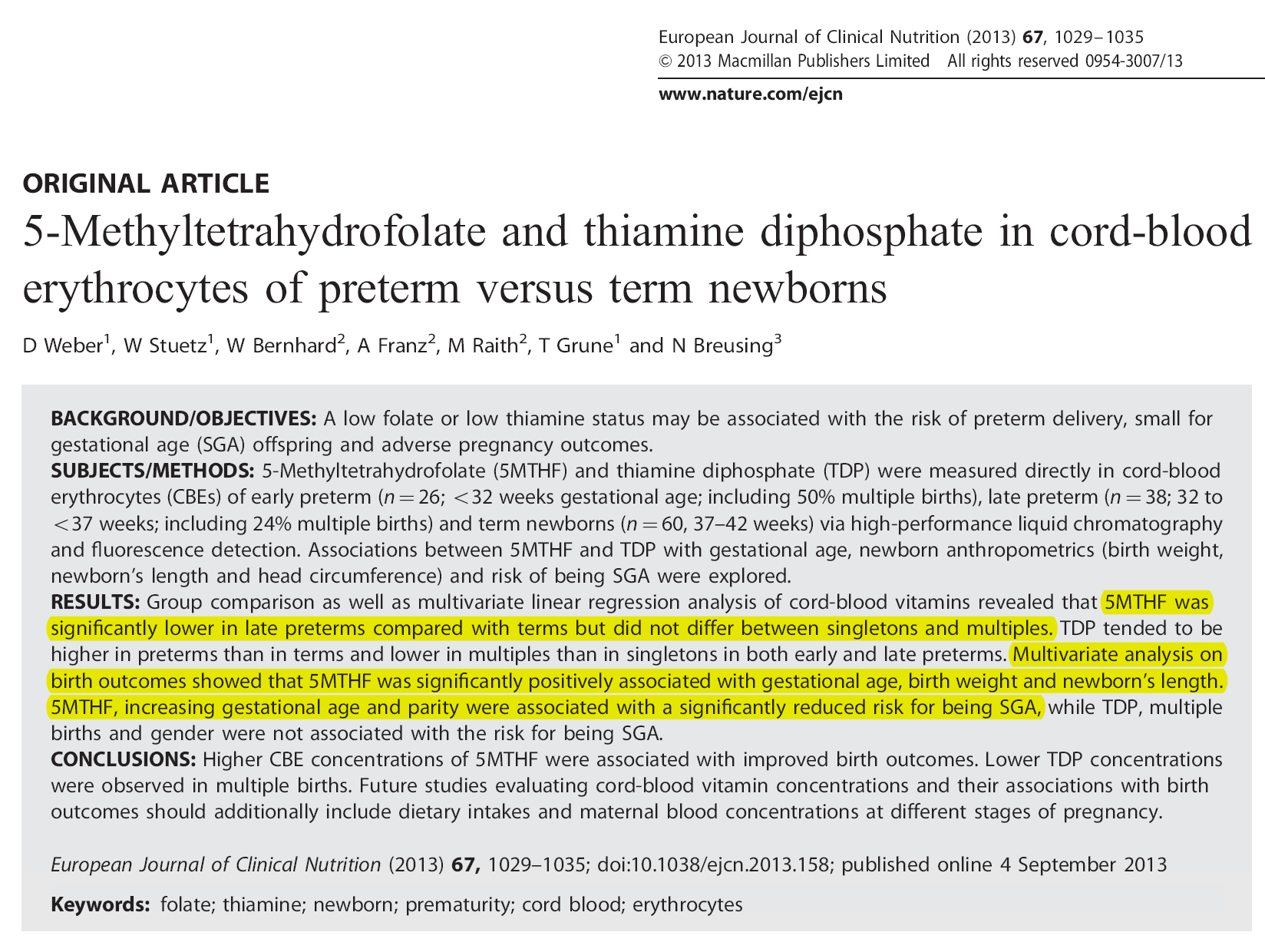
This directly relates to three key prenatal indicators: gestational age, birth weight, and body length.
Conversely, infants with lower 5-MTHF levels were more likely to be small-for-gestational-age.
Simply put, despite reaching the corresponding gestational week, the baby’s weight and development lag far behind peers.
Such infants may face feeding difficulties, weaker immunity, and greater challenges in catching up in growth after birth.
The study also suggested that higher 5-MTHF levels combined with longer gestation, along with a prior pregnancy history, may correlate with a lower risk of SGA.
Even a prior pregnancy does not guarantee safety.
Fetal development is influenced by multiple factors.
Maternal health affects nutrient metabolism; previous pregnancy history and placental function both play roles.
I was surprised by these findings.
Previously, when I thought of folate, my first thought was taking it during preconception and early pregnancy to prevent neural tube defects.
This study reminds us that folate is involved in fetal growth and development throughout pregnancy.
The causes of preterm birth and SGA are complex.
Folate status, especially 5-MTHF levels, may be an easily overlooked factor.
This raises another question: some people cannot utilize ingested folate with equal efficiency.
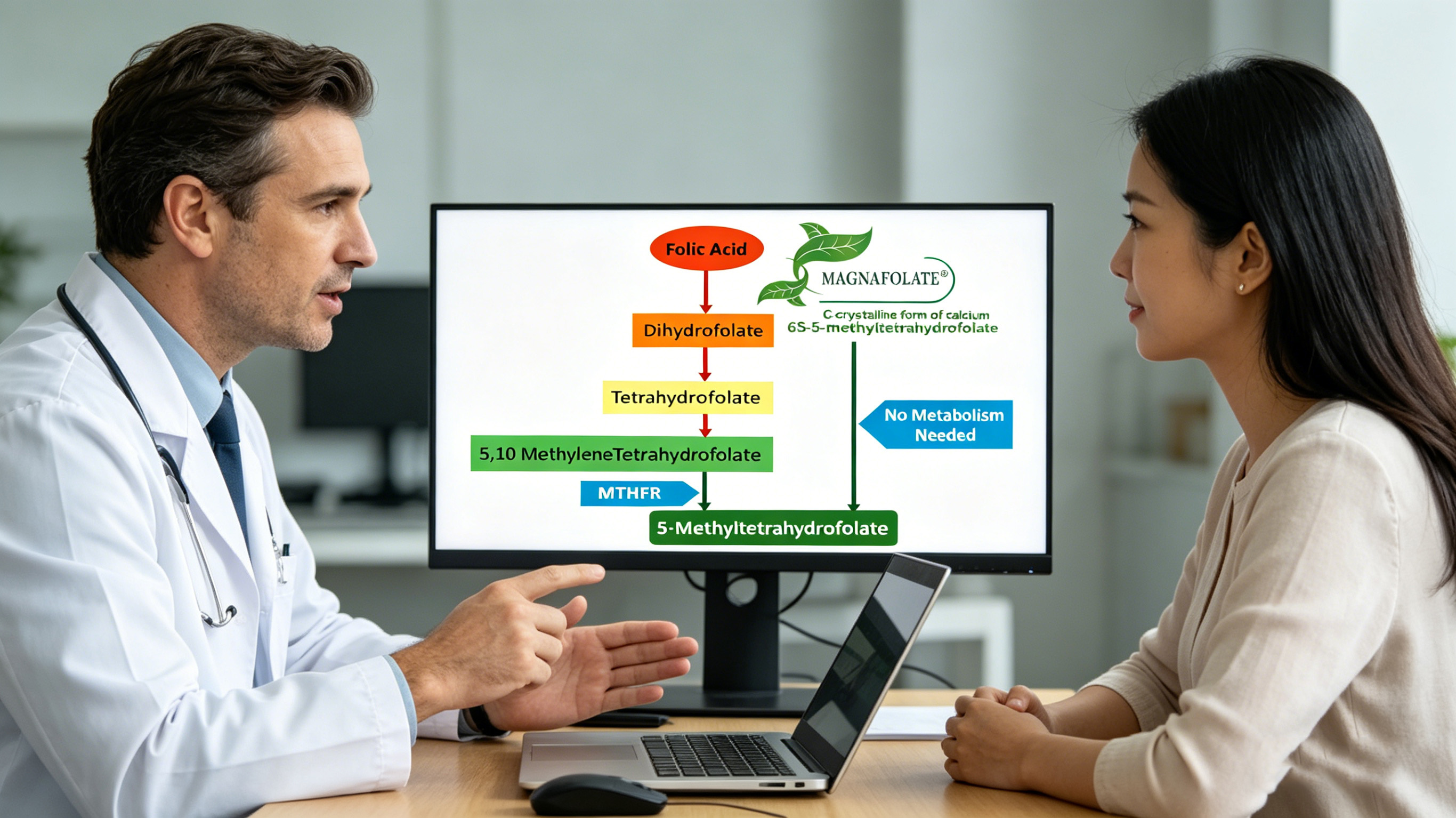
Most common folic acid tablets are synthetic.
Synthetic folic acid requires a series of metabolic conversions in the body to become 5-MTHF, the biologically active form that functions effectively.
For most people, standard supplementation with synthetic folic acid is still beneficial.
However, its effectiveness may be reduced in those with metabolic inefficiency.
MTHFR gene polymorphism is frequently cited as a factor affecting conversion efficiency.
Some individuals have variants in the MTHFR gene, leading to reduced enzyme activity.
As a result, the conversion of synthetic folic acid to 5-MTHF becomes less efficient.
Data indicate that MTHFR gene variants are common in the general population, with varying prevalence across regions and ethnic groups.
With low conversion efficiency, ingested folic acid cannot be fully converted into the needed 5-MTHF.
Some individuals also have elevated homocysteine (Hcy) levels.
This is disadvantageous for pregnant women: they take folic acid regularly but fail to achieve the desired effect due to metabolic differences.
Folic acid supplementation depends on whether the body can use it effectively.
This is where active folate has an advantage.
Calcium 6S-5-methyltetrahydrofolate is the 5-MTHF form.
This ingredient does not rely on MTHFR enzyme conversion and can be directly absorbed. For the 78.4% of the Chinese population with MTHFR-related folate metabolic disorders, active folate may be more effective.
However, active folate has a technical challenge: stability.
5-MTHF is sensitive to moisture, high temperatures, and oxygen; poor raw materials or processing can lead to degradation during storage, producing harmful impurities such as JK12A.
In short, the quality of active folate depends on its storage stability.
I researched sources of active folate and found a C-crystal form ultrasonic crystallization technology that forms a protective layer around fragile molecules, reducing degradation over time.
According to manufacturer disclosures, this patented C-crystal form (Magnafolate) remains stable for over three years at room temperature, ensuring active folate tablets stay effective throughout their shelf life.
How can ordinary pregnant women determine if they need active folate?
If folate status is suboptimal in preconception or prenatal tests, or if homocysteine (Hcy) is elevated due to abnormal folate metabolism markers, or if there is folate metabolic risk, discuss with a doctor about adjusting the folate form.
Specific dosage, duration, and supplementation plan should always follow professional medical advice.
Finally, it must be clarified: folate is important but cannot solve all problems.
Anxiety during pregnancy often comes not from “not knowing” but from “knowing but being unable to act.”
Terms like folate, preterm birth, and SGA seem distant until they affect someone close.
We don’t need to be experts—just two things: keep regular prenatal checkups and ask questions.
Even five more minutes of conversation with a doctor is better than scaring yourself.
The fact that you’re reading this article carefully means you’re already doing great.
References
[1] 5-Methyltetrahydrofolate and thiamine diphosphate in cord-blood erythrocytes of preterm versus term newborns. *European Journal of Clinical Nutrition*, 2023 Oct. DOI:10.1038/s41430-023-01347-y
[2] Lian Zenglin, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological Characteristics and Applications of Folic Acid and 5-Methyltetrahydrofolate. *China Food Additives*, 2022(2).
Disclaimer
Magnafolate is supplied only as a raw material for calcium 6S-5-methyltetrahydrofolate (active folate) and is not intended for direct diagnostic or therapeutic use by consumers. Any supplementation decisions should be made under professional medical guidance.
The story in this article is fictionalized based on common scenarios and research cases to convey scientific information, not representing real individual experiences. This product is a food raw material and is not a substitute for medicine.


 Online Service
Online Service
