
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






George Zhou had been taking folate for six weeks, yet his blood vessels did not seem to improve much. So where was the problem?
George is 72 this year. Three years ago, he had a coronary angiography. The report showed atherosclerotic narrowing of the coronary arteries. He took his prescribed medications regularly, and his blood pressure stayed fairly stable. When he walked for too long, his chest would feel tight. After a short rest, it eased. He never thought much of it. This time, his checkup report showed one extra number: homocysteine, 16.8 μmol/L. His folate level was also on the low side. The doctor suggested he add folate supplementation.
Six weeks later, George went back for a follow-up. His homocysteine had dropped, and the chest tightness during walking happened less often. He was pleased. Finally, he thought, he had found the right direction. Then the doctor said something during the visit. “You feel better. Now let’s see whether the elasticity of your blood vessels has improved.”
George froze. “Wait a minute. If the number improved, shouldn’t my body improve right along with it?”
52 Patients With Coronary Heart Disease: Folate Changed FMD
In July 2001, *ATVB* published a study that looked at exactly this issue. The study included 52 patients with coronary artery disease. It used a randomized, double-blind, placebo-controlled crossover design. Participants took 5 mg of folate every day for six weeks. The researchers focused on one hard endpoint: flow-mediated dilation, or FMD. FMD is used to assess vascular endothelial function. The endothelium is the thin inner lining of blood vessels, and it helps control how well blood vessels relax. After folate treatment, plasma folate levels increased (P < 0.001), homocysteine fell by 19% (P < 0.001), and FMD also improved (P < 0.001). Folate went up. Homocysteine went down. Vascular function improved.
So far, the story sounds straightforward. But there was one big problem in the data. The degree of FMD improvement had no correlation with the degree of homocysteine reduction.
Homocysteine Went Down, But That Wasn’t the Whole Story
The usual explanation goes like this: elevated homocysteine can damage the vascular endothelium. Folate helps metabolize homocysteine, so the blood vessels should naturally feel better. But the ATVB study suggested that the picture was not that simple. In the study, folate lowered homocysteine. Yet MDA did not change, and neither did TAOC. MDA reflects lipid peroxidation, while TAOC reflects total antioxidant capacity. In other words, plasma-level markers of oxidative stress did not really move. If the drop in homocysteine were the reason folate improved vascular function, then the improvement in FMD should have tracked with the fall in homocysteine. The data did not support that assumption. The researchers realized the old pathway was not enough to explain what they were seeing.
5-MTHF Entered the Blood Vessel — And Acted Fast
The researchers then ran a second experiment. Another 10 patients with coronary heart disease received 5-methyltetrahydrofolate, or 5-MTHF, directly through intra-arterial infusion at a dose of 50 μg/min. This bypassed oral absorption and liver metabolism. The active folate was delivered straight to the local blood vessel. FMD improved (P < 0.001). Then they measured homocysteine again. Surprisingly, it did not change (P = 0.47). Homocysteine did not fall, yet vascular dilation improved. That finding pointed to an independent pathway: 5-MTHF could act directly on the endothelium. The researchers then turned their attention to intracellular superoxide. Superoxide is a type of reactive oxygen species. When too much of it builds up inside cells, it reacts with nitric oxide and consumes it. Blood vessel relaxation depends on nitric oxide to transmit the signal. Once that signal is depleted, the vessel’s response becomes sluggish. The endothelium controls vascular relaxation. Nitric oxide carries the relaxation signal. Superoxide consumes that signal. The blood vessel then responds a step too late.
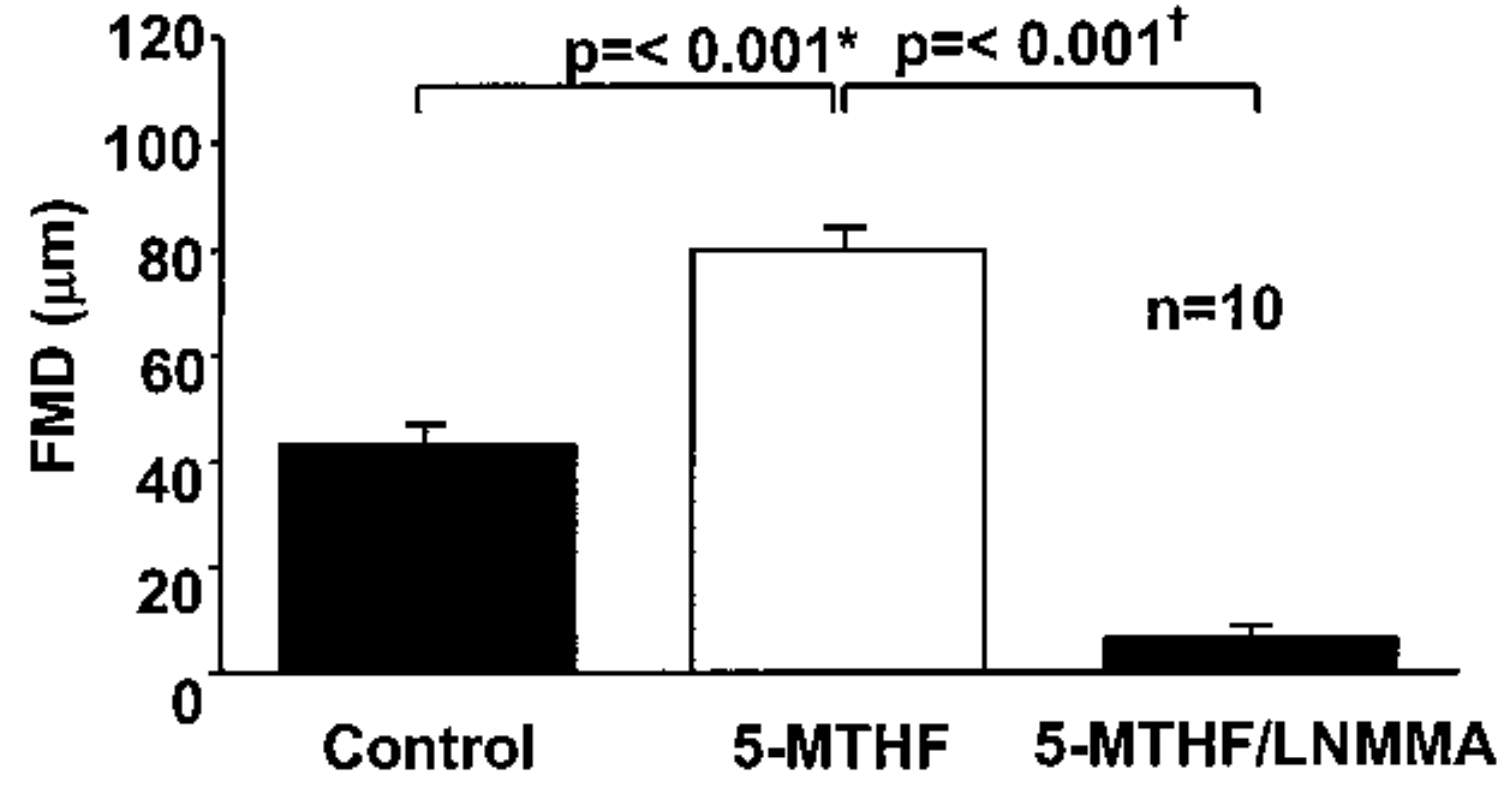
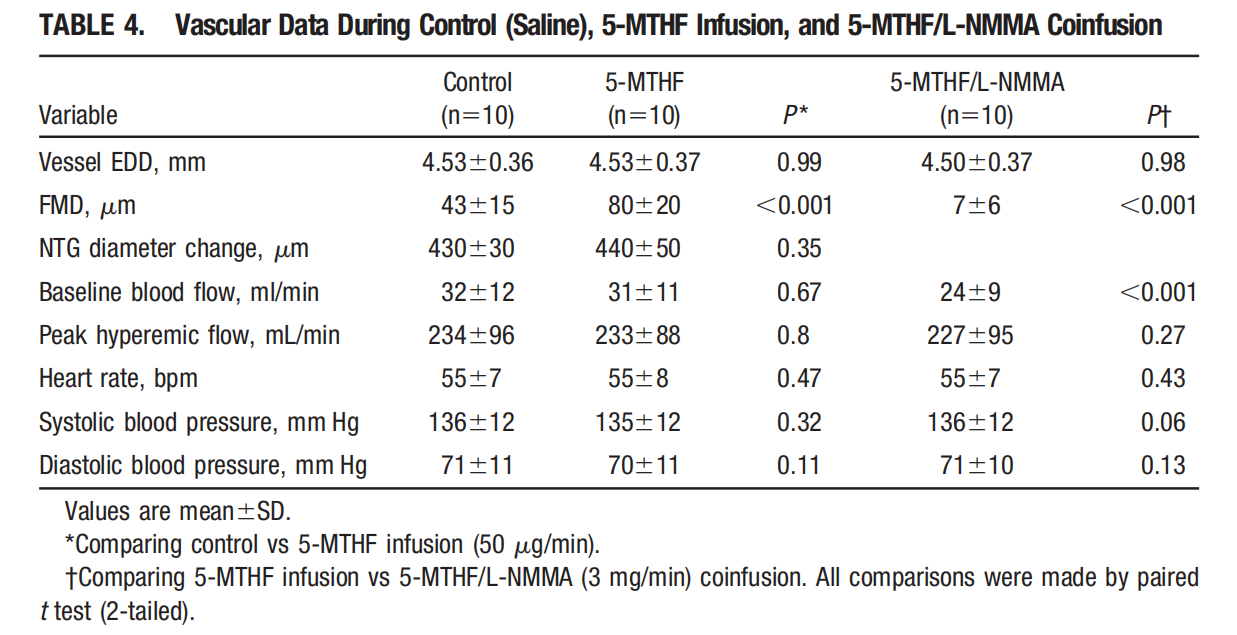
Oxidative Pressure Inside the Cell Was the Hidden Variable
The in vitro experiments made the clue much clearer. Homocysteine induced an increase in superoxide inside endothelial cells. When 5-MTHF was added, that increase disappeared (P < 0.001). The clinical observations and cell experiments finally matched. 5-MTHF did not wait for homocysteine to fall. It directly influenced endothelial function. By reducing intracellular superoxide, it helped nitric oxide keep doing its job. The researchers proposed several possible mechanisms: directly scavenging superoxide, increasing nitric oxide produced by eNOS, or reducing superoxide generated by eNOS itself. Which pathway dominates in the human body still needs more research. But the direction became much more specific: the value of folate is not limited to the Hcy number in plasma. Part of its effect may happen inside endothelial cells.
There Is a Conversion Barrier Between Regular Folate and Active Folate
When folate is taken orally, it cannot immediately be used as 5-MTHF. Regular synthetic folic acid must go through several metabolic steps before it becomes the active form commonly used by the body. One key enzyme in this process is MTHFR. MTHFR gene polymorphisms are common in the Chinese population. Data from Chinese Han adults published in *PLoS ONE* in 2013 showed regional differences in the frequency of the TT homozygous mutation at the C677T site. For people who need to manage homocysteine levels, the efficiency of this enzyme can strongly affect how well regular folic acid is converted into its active form. That is why the form matters.
Active folate can bypass the MTHFR step and enter the one-carbon metabolism cycle in the form of 5-MTHF. For people with lower MTHFR metabolic efficiency, this pathway helps folate reach where it is supposed to go. Among raw materials on the market that provide the calcium salt form of 6S-5-MTHF, Magnafolate is one option. As an active folate raw material of calcium 6S-5-methyltetrahydrofolate, it avoids the MTHFR-dependent step involved in converting regular folic acid into 5-MTHF. For people who need to manage folate status and homocysteine levels under the guidance of a doctor or nutritionist, the form of the raw material becomes a key variable.
The Supplementation Logic Has Changed. The Markers We Watch Should Change Too.
For years, discussions about folate and cardiovascular health focused almost entirely on homocysteine. Elevated Hcy is associated with cardiovascular risk, and folate participates in its metabolism. The ATVB study pushed the discussion one layer deeper. Improvement in vascular endothelial function may appear before homocysteine has fully come down, and it may occur through pathways beyond homocysteine itself. When looking at cardiovascular health, we need more than one number. Folate level, homocysteine, underlying diseases, medication use, kidney function, blood pressure, blood lipids, and possible MTHFR-related metabolic differences can all shape the supplementation strategy. Active folate provides another pathway, but it does not replace clinical treatment. Active folate raw materials such as calcium 6S-5-MTHF, including Magnafolate, offer a basis for choosing a form closer to what the human body can use. They may serve as a reference at the raw-material selection level, but they should not be understood as a disease intervention plan. That boundary has to stay clear.
George Changed What He Paid Attention To
Later, under his doctor’s advice, George stopped looking at folate supplementation through a single number. Instead, he began tracking a group of indicators. Three months later, at his follow-up visit, his homocysteine remained at a lower level. The doctor shifted the focus of evaluation to blood pressure, blood lipids, exercise tolerance, and endothelial function. George finally got it. The numbers on a checkup report are not the whole map.
The Next Layer of Folate’s Value Is Inside the Cell
What the ATVB study added was a deeper explanation. Folate’s improvement of endothelial function in patients with coronary heart disease is related to homocysteine metabolism, but it should not be reduced to a single cause-and-effect chain. 5-MTHF improved FMD and reduced superoxide inside endothelial cells. That gives active folate another cell-level explanation for its role in vascular health. For the general population, under professional guidance, folate form, metabolic capacity, and follow-up markers should be reviewed together. Active folate raw materials such as calcium 6S-5-MTHF, including Magnafolate, provide a form closer to what the body can use and may help manage folate nutritional status. Any supplementation decision still has to come back to individual assessment.
References
[1] Doshi S. N., McDowell I. F. W., Moat S. J., et al. Folate Improves Endothelial Function in Coronary Artery Disease: An Effect Mediated by Reduction of Intracellular Superoxide[J]. *Arteriosclerosis, Thrombosis, and Vascular Biology*, 2001, 21(7): 1196–1202. doi:10.1161/hq0701.092000.
[2] Yang B., Liu Y., Li Y., et al. Geographical Distribution of MTHFR C677T, A1298C and MTRR A66G Gene Polymorphisms in China: Findings from 15,357 Adults of Han Nationality[J]. *PLoS ONE*, 2013, 8(3): e57917. doi:10.1371/journal.pone.0057917.
[3] Lian Zenglin, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological Characteristics and Applications of Folic Acid and 5-Methyltetrahydrofolate. *China Food Additives*, 2022, Issue 2.
Risk Notice
Magnafolate is supplied only as an active folate raw material of calcium 6S-5-methyltetrahydrofolate. It is not intended to provide diagnostic or treatment advice directly to consumers. Any decision about folate supplementation should be made under the guidance of a qualified doctor or nutritionist.
The person described in this article is a fictional case, used only to help readers understand the scientific mechanism. The story details and data fall within commonly seen clinical reference ranges. The causal discussion in this article is limited to conclusions supported by the cited literature and does not constitute a promise of efficacy for any product.


 Online Service
Online Service
