
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






“Taking folic acid when preparing for pregnancy” is common advice for most expectant parents. But did you know that not everyone is suited to the commonly used folic acid? For couples affected by MTHFR gene polymorphism, choosing the wrong form of folate may not only be ineffective but could also increase the risk of infertility and miscarriage.
Globally, about 48.5 million couples face infertility, and among them, MTHFR gene polymorphism is an easily overlooked yet critical factor.
A 2023 Australian case series study published in Exploratory Research in Clinical and Social Pharmacy focused on this issue, providing important insights for folate supplementation in people with MTHFR gene polymorphism. Today, we’ll discuss “personalized” folate choices during preconception, especially for those struggling with infertility or diagnosed with MTHFR variants.
First, what is MTHFR gene polymorphism?
Simply put, MTHFR is a key enzyme in the human body responsible for converting folate into its active form. When the MTHFR gene undergoes variants (such as the common C677T or A1298C), the enzyme’s activity decreases, making it difficult to efficiently convert the folic acid we usually take into the body’s usable active folate (6S-5-methyltetrahydrofolate, 5-MTHF). This leads to folate metabolism impairment, which can affect follicle development, sperm production, and embryo quality, increasing the risk of infertility and recurrent miscarriage.

Previously, many national health policies, including Australia’s, recommended that women of childbearing age supplement with folic acid. However, this study found that for infertile women carrying MTHFR gene polymorphism, such a “one-size-fits-all” recommendation may not be appropriate.
What did the study find?
The study included 12 patients, 83.3% of whom had a history of miscarriage and 41.7% had experienced failed assisted reproductive cycles. All were diagnosed with MTHFR gene polymorphism (most commonly C677T heterozygous, compound heterozygous, etc.). For these women, every negative pregnancy test was more than just a number—it represented emotional and physical exhaustion. Finding a truly suitable nutritional plan became urgent.
Notably, the six experienced clinicians involved (average practice experience over 20 years) instructed all patients to stop taking any supplements containing folic acid and switched them to prescriptions of 6S-5-methyltetrahydrofolate (5-MTHF) alone or combined with folinic acid. More importantly, the average maximum daily dose of prescribed 5-MTHF reached 2325 µg—far higher than the standard recommendation of 400–500 µg—and was adjusted according to genotype:
- C677T heterozygous patients: 500–3800 µg/day (average 2850 µg)
- Compound heterozygous patients: 1500–3800 µg/day (average 2400 µg)
- The only C677T homozygous patient: 3500 µg 5-MTHF + 700 µg folinic acid
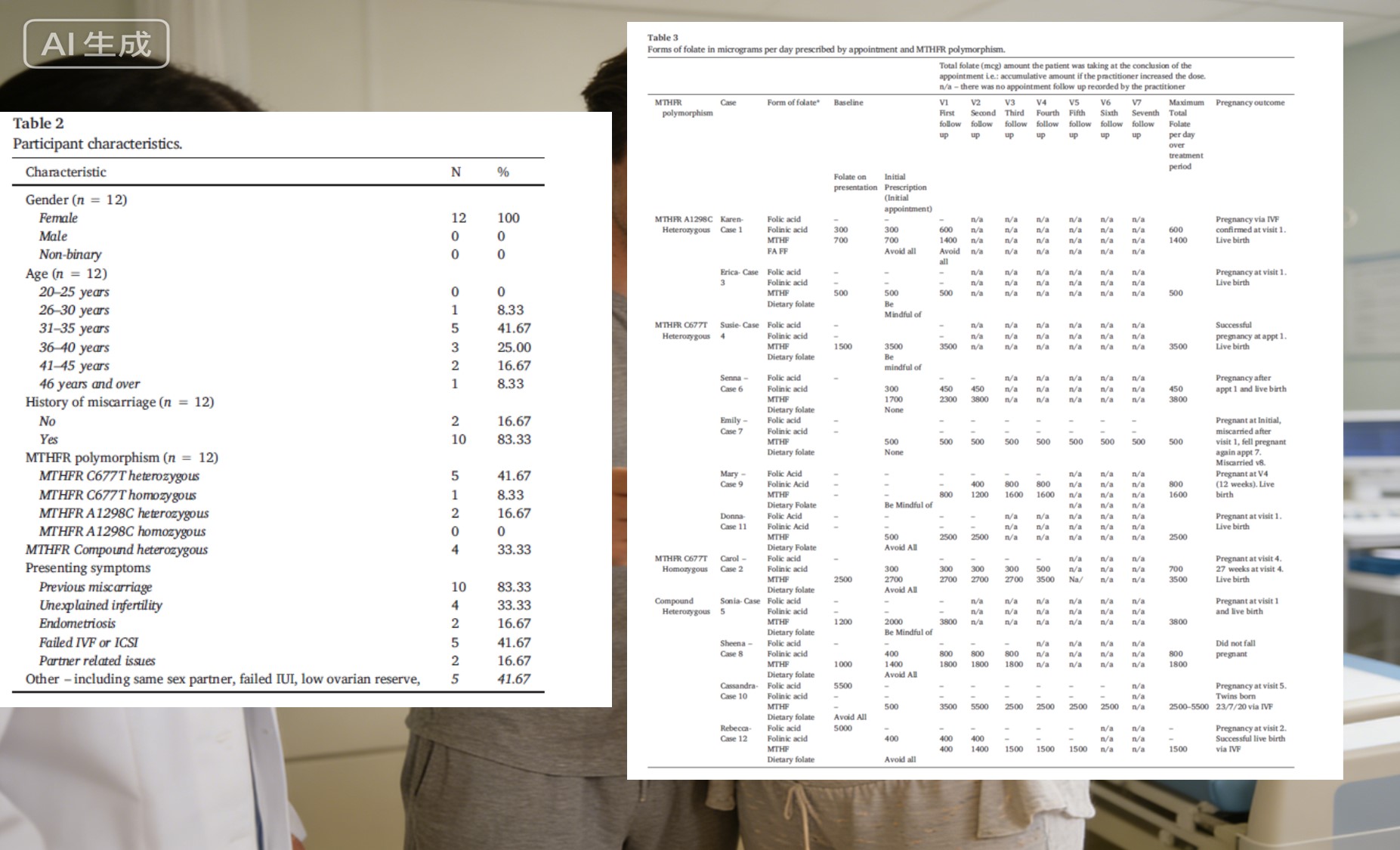 The clinical outcomes were encouraging: 11 of the 12 patients conceived
within an average one-year treatment period, with 10 resulting in live births.
All who conceived started taking non‑folic-acid supplements (mainly 5-MTHF) and
achieved pregnancy within 2–4 months. Importantly, patients tolerated the
5-MTHF well; only one reduced dosage due to anxiety at high dose.
The clinical outcomes were encouraging: 11 of the 12 patients conceived
within an average one-year treatment period, with 10 resulting in live births.
All who conceived started taking non‑folic-acid supplements (mainly 5-MTHF) and
achieved pregnancy within 2–4 months. Importantly, patients tolerated the
5-MTHF well; only one reduced dosage due to anxiety at high dose.
From research to practice: The significance of personalized folate supplementation
This study reinforces our belief that for women with MTHFR gene polymorphism, “bypassing metabolic obstacles and directly supplementing active folate” is not only scientifically sound but also reduces ineffective attempts and boosts confidence.
As a patented Crystal Form C active folate with actual non-toxic safety, Magnafolate can rapidly raise serum and red blood cell folate levels, helping the body reach the ideal preconception state faster. It is produced without toxic reagents such as formaldehyde or p-toluenesulfonic acid, making it more suitable for women during preconception, pregnancy, and lactation.
Every family trying to conceive experiences long periods of hope and anxiety, especially those who have suffered miscarriages or assisted reproductive failures—they need precise nutritional support rather than “blind supplementation.”
Magnafolate, grounded in scientific research and innovation, delivers stable, safe, and precise active folate to every family in need, helping smooth the path to welcoming new life.
Conclusion
Every step on the road to conception deserves care and attention.
Magnafolate aims to build on solid scientific foundations, working with clinical experts, doctors, and expectant parents to continuously explore finer gene-nutrition solutions, so that science and compassion go hand in hand, accompanying you steadily toward the arrival of new life.
Risk notice:
This study had a small sample size and limited evidence level; conclusions
require validation through higher-quality studies. Folate supplementation
should be individualized and conducted under the guidance of a doctor or
pharmacist. Do not self-prescribe high doses.
References
[1] Variations in folate prescriptions for patients with the MTHFR genetic
polymorphisms: A case series study. Exploratory Research in Clinical and
Social Pharmacy, 2023.
[2] Lian Zenglin, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological
characteristics and applications of folic acid and 5-methyltetrahydrofolate. China
Food Additives, 2022(2).


 Online Service
Online Service
