
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






59-year-old Aunt Wang, a retired primary school Chinese teacher, used to walk briskly and enjoy good health.
One cold winter day last year, she bent down to pick up a key. As she stood up, a sharp pain shot through her lower back. A hospital X-ray revealed a lumbar compression fracture, with a bone mineral density T-score of -2.8.
She was stunned. “I’ve been taking calcium supplements all along—how could this happen…?”
After reviewing the report, her doctor didn’t discuss calcium pills. Instead, he asked: “Have you checked your homocysteine level?”
She had never heard of this marker.
“Your Hcy is elevated. This isn’t just a cardiovascular issue—it affects your bones too.”
Osteoporosis Is Not Just Calcium Deficiency
Most people think osteoporosis means simply not getting enough calcium. But bone is not like concrete that stays fixed once poured. It is constantly being broken down and rebuilt—osteoclasts break down old bone, osteoblasts build new bone. The balance between these two processes determines bone strength.
Doctors typically monitor two key markers of this balance:
- Osteocalcin (OC): A byproduct of osteoblast activity; higher levels mean active bone formation.
- β-CTx: A breakdown product of bone collagen; higher levels indicate accelerated bone loss.
When breakdown outpaces formation, bones gradually become brittle.
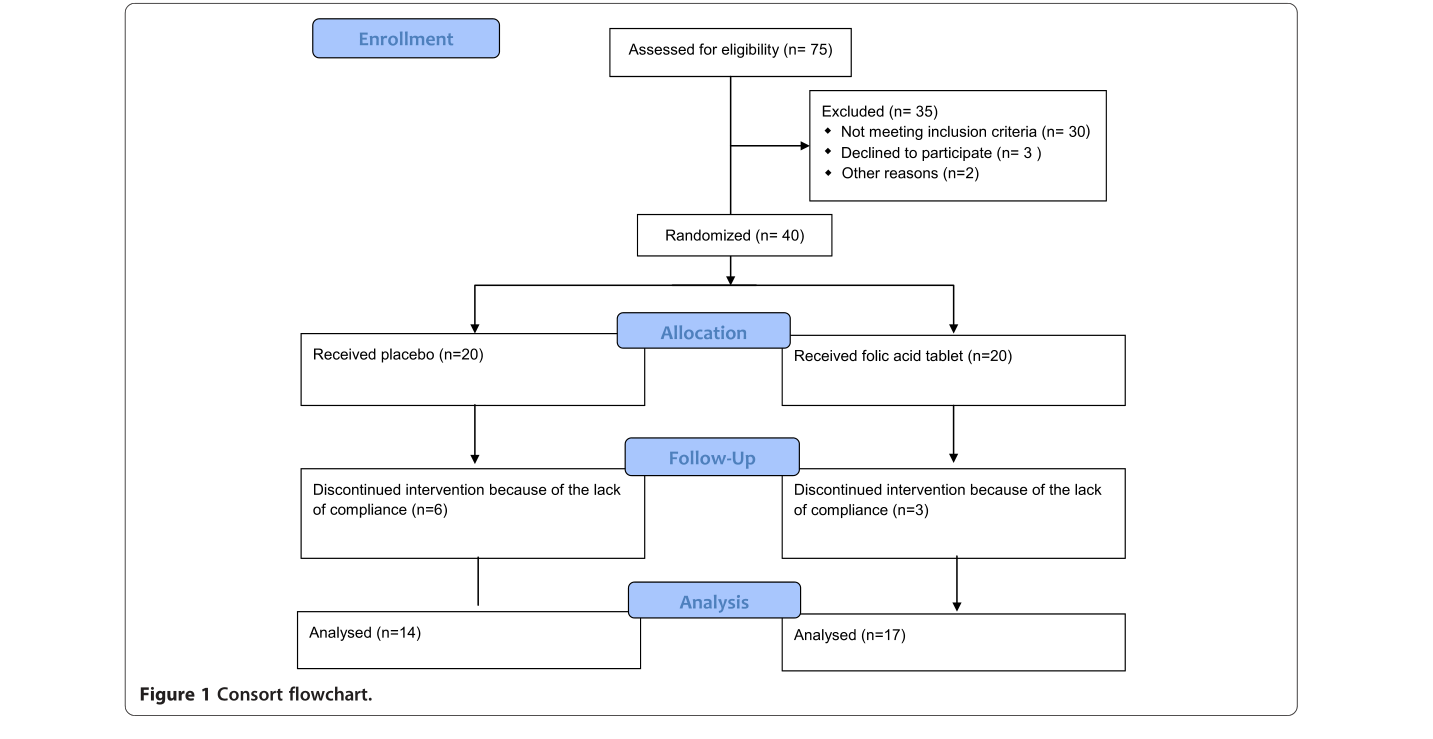
In 2014, an Iranian research team published a randomized, double‑blind trial in the *DARU Journal of Pharmaceutical Sciences* (IF 4.088 at the time) examining folic acid’s effects on postmenopausal women with osteoporosis. Forty participants were enrolled: 17 in the folic acid group and 14 in the placebo group (some dropped out). They were followed for 6 months.
After 6 months, significant differences emerged between the two groups in osteocalcin and β‑CTx (P ≤ 0.05). The folic acid group showed more favorable bone metabolism markers, and changes in Hcy levels correlated with bone turnover rates.
In short: Folate → lowers Hcy → benefits bone health. The research team discussed this mechanistic pathway in detail.
When folate intake is insufficient, homocysteine cannot be metabolized normally and accumulates. Elevated Hcy impairs osteoblast function and disrupts collagen cross‑linking in bone—sometimes bones become brittle not from calcium deficiency, but from faulty “glue.”
Postmenopausal women face a sharp drop in estrogen, which slows folate metabolism. Combined with poor dietary intake, this makes elevated Hcy far more common than in younger women.
Taking Folic Acid Pills Daily May Not Help
You might think: Just take a bottle of folic acid tablets, right?
Not necessarily.
The inexpensive folic acid sold in pharmacies is mostly synthetic (oxidized folic acid). After ingestion, the body must convert it step by step into its biologically active form: 5‑methyltetrahydrofolate (5‑MTHF). This is like buying flour and having to knead dough and steam buns before you can eat it.
The problem lies in this conversion process. The key enzyme is MTHFR, and gene variants of this enzyme are common in Chinese populations—about 40%–60% carry some variant. Gene variants reduce conversion efficiency: you may take plenty of folic acid, but little becomes usable, and Hcy remains high.
Therefore, more researchers and clinical nutritionists now recommend: instead of supplementing with folic acid and waiting for the body to convert it, use the pre‑converted active form—Calcium 6S‑5‑MTHF. It requires no conversion, is immediately usable, and works regardless of genetics.
One reliable domestic manufacturer of this ingredient is Lianyungang Jinkang Hexin Pharmaceutical Co., Ltd. Their Magnafolate® uses a patented C crystal process, with the active ingredient being Calcium 6S‑5‑MTHF. The biggest challenge for active folate is not efficacy but stability—it degrades easily. Magnafolate® achieves 48 weeks of stability at room temperature, solving a key formulation challenge. Safety studies confirm it is practically non‑toxic.
Research suggests supplementation with Calcium 6S‑5‑MTHF effectively increases serum and red blood cell folate levels and helps lower homocysteine—directly supporting the “lower Hcy → protect bone” pathway.
Risk Disclosure
Limitations of the cited study include: small sample size (31 completed participants), 6‑month follow‑up, and no subgroup analyses by age or gender. The authors themselves noted that larger, longer studies are needed for confirmation.
Currently, we can confirm a trending association between folate supplementation and bone metabolism markers, but we cannot conclude that “folate cures osteoporosis.”
Osteoporosis is a systemic condition related to calcium, vitamin D, exercise, hormone levels, genetics, and more. Folate is only one component.
If you have abnormal bone density, consult a doctor for a full evaluation and follow medical advice.
Magnafolate® is supplied only as a raw material (Calcium 6S‑5‑MTHF) and does not provide diagnostic or therapeutic advice directly to consumers. Any supplementation decisions should be made under professional medical guidance.
Purpose of This Article
While reviewing folate literature, I found limited domestic attention to the link between folate and skeletal health; most research focuses on birth defects and cardiovascular disease. However, the 2014 *DARU* trial data merits discussion, especially for postmenopausal women.
For postmenopausal women with elevated Hcy, considering folate status as part of skeletal health management—after medical evaluation—is supported by literature. Active folate offers theoretical advantages because it does not depend on MTHFR conversion, although “theoretical” requires further clinical validation.
If this article reminds you of yourself or an elder, consider two simple steps: get a bone density test and a homocysteine test. It takes minutes, but knowledge is better than uncertainty.
Note: The story in this article is fictional, based on common scenarios and research cases, for scientific communication only. This product is a food ingredient and is not a substitute for medicine.
References
[1] Lian Zenglin, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological Characteristics and Applications of Folic Acid and 5‑Methyltetrahydrofolate. *China Food Additives*, 2022(2).
[2] Golbahar J, Hamidi A, Aminzadeh MA, Omrani GR. Effect of folic acid on bone metabolism: a randomized double blind clinical trial in postmenopausal osteoporostic women. *DARU Journal of Pharmaceutical Sciences*, 2014, 22(1). DOI: 10.1186/2008‑2231‑22‑1


 Online Service
Online Service
