
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






After getting his physical examination report, Lao Ye immediately focused on the exceeding number: homocysteine 18.6 μmol/L.
The cardiologist glanced at the lab sheet.
"Go back and take folic acid. This is common; the index will usually go down with adequate supplementation."
Lao Ye followed the advice carefully, bought several boxes of folic acid tablets, took one after breakfast every day, and never missed a day for three months.
On the recheck day, he got the report: 17.2.
Still above the standard. After nearly 100 days of supplementation, it only dropped by 1.4.
Lao Ye sat on the bench in the hospital corridor, holding the sheet, wondering if the medicine was ineffective or his body had problems.
He decided to search for information online.
Along the search results, he found a term he had never noticed before:
Red blood cell 5-methyltetrahydrofolate.
Next to it was a sentence that made him pause the mouse for a long time: Red blood cell 5-MTHF level is a more accurate cardiovascular and metabolic indicator than homocysteine.
What does this mean?
Simply put, the folic acid you take may not actually be used by your body.
Many people know that high homocysteine is bad and a hidden danger to cardiovascular health, but few people think about one question: Where does Hcy come from and what removes it?
Lao Ye hadn't thought about it before either.
How Hcy is produced
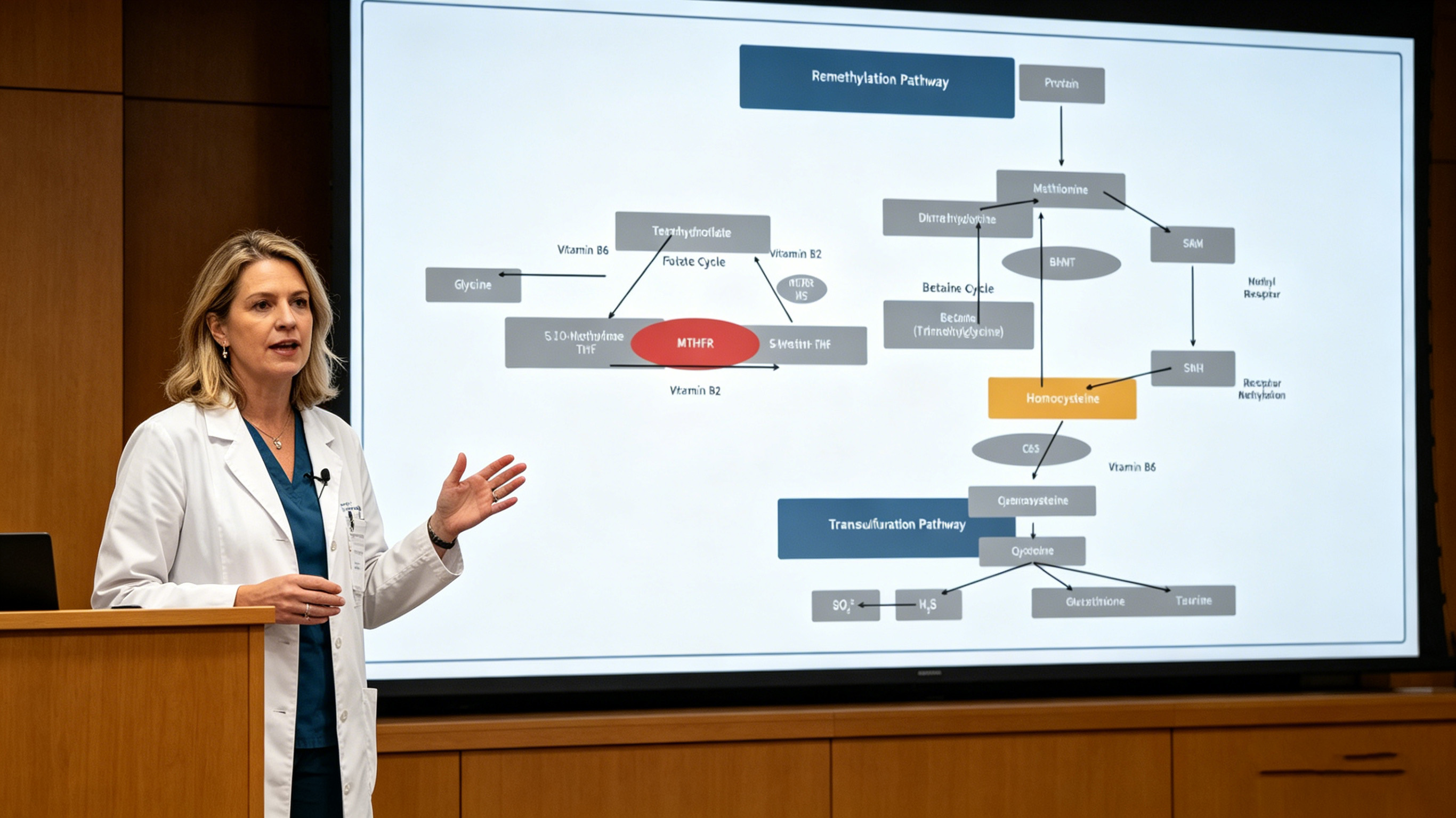
During protein metabolism, the human body produces a metabolic byproduct called homocysteine.
Under normal conditions, the body processes it promptly through a process called remethylation — converting Hcy into harmless methionine so it can re-enter metabolism.
This process requires a key ingredient: 6S-5-methyltetrahydrofolate (5-MTHF).
Note this name; it will be mentioned repeatedly later.
The problem is: whether folate comes from spinach or over-the-counter tablets, it does not exist as 5-MTHF. After entering the body, it must first be processed into usable 5-MTHF.
The enzyme responsible for this processing is called MTHFR.
And this is precisely where the biggest individual differences lie.
Your body's "folic acid factory" may not be efficient enough
Insufficient MTHFR enzyme activity usually has three causes:
First, genetics. People with specific genetic variants naturally have lower enzyme efficiency. This is not rare in the Chinese population, though most have not been tested.
Second, age. Enzyme activity declines with age — a natural law no one can avoid.
Third, nutritional status. Enzyme function is limited when the body lacks certain trace elements. What is lacking? Explained later.
The three factors act alone or in combination, leading to the same result:
Ordinary folic acid is ingested but not efficiently converted into 5-MTHF.
The active folate available in red blood cells to clear Hcy remains insufficient. Thus Hcy stays high — even if you have taken a lot of folic acid.
After reading this, Lao Ye closed the webpage and thought for a long time.
He suspected this was his case: he took plenty of pills, but folic acid just passed through his body without working much.
Is there supporting research data?
Yes.
In December 2012, the journal *High Blood Pressure & Cardiovascular Prevention* published a community study. Researchers investigated more than 900 adults and did three things:
1. Measured blood pressure
2. Measured plasma homocysteine (Hcy)
3. Measured 5-MTHF content in red blood cells
The results were striking.
Among men, the group with the lowest red blood cell 5-MTHF levels had 1.8 times the risk of hypertension compared to the group with the highest levels.
Simply due to different active folate levels in red blood cells, cardiovascular risk nearly doubled.
The researchers wrote a straightforward statement in the report:
Red blood cell 5-MTHF is more reliable than plasma Hcy; it reflects the real status of folate metabolism.
In plain language: High Hcy is already a fire, while low red blood cell 5-MTHF is a smoke signal detected earlier.
Intervening after Hcy exceeds the standard is already one step too late. The real early warning is upstream.
What about women?
The study found this pattern did not appear in women.
The researchers explained: hormonal backgrounds differ between men and women, folate metabolic pathways vary, and cardiovascular diseases develop differently.
In other words, this issue is particularly important for middle-aged men.
If you know someone — over 40, with high Hcy in physical exams, and ineffective folic acid supplementation — this article is worth sharing with them.
So what to do?
Back to Lao Ye's problem.
He now understands: the daily folic acid tablets he took likely could not be fully converted into functional 5-MTHF due to insufficient MTHFR enzyme efficiency.
Is there a way to skip the conversion step?
Yes.
There is a form of folate that does not require MTHFR processing and can directly participate in Hcy remethylation after entering the body. Its full name is calcium 6S-5-methyltetrahydrofolate, also called active folate.
By skipping the conversion step, it is absorbed and utilized faster and more directly.
In the domestic active folate raw material field, Magnafolate supplies exactly this calcium 6S-5-methyltetrahydrofolate. Chemically, it matches the active folate produced by human metabolism. In other words, the body can use it directly without further conversion.
This is why many people who find ordinary folic acid ineffective see Hcy decrease after switching to active folate — it is not a matter of insufficient dosage, but of mismatched form.
An information gap
What took Lao Ye nearly four months to understand can be condensed into one sentence:
People usually only monitor Hcy to judge folic acid supplementation effects, but do not know that upstream in the metabolic process, there is an earlier indicator — red blood cell 5-MTHF.
For people like Lao Ye who take supplements regularly but see little change in rechecks, the core reason is most likely not insufficient intake, but failure to convert what is ingested.
The 2012 study confirms this: long before blood pressure problems arise, folate metabolism is already abnormal in many people. No one just tells them which index to check.
Understanding this is not to cause anxiety, but to make nutritional supplementation targeted and effective.
Final note
Dosage of active folate supplementation varies individually. People with hypertension or high Hcy are advised to develop a personalized plan after professional medical evaluation. If taking medications such as methotrexate, consult a doctor before supplementation due to potential interactions.
As a supplier of calcium 6S-5-methyltetrahydrofolate (active folate) raw materials, Magnafolate does not provide diagnosis or supplementation advice directly to consumers. For specific plans, follow medical advice.
References
[1] Association between Low Red Blood Cell 5-Methyltetrahydrofolate and Hyperhomocysteinaemia with Hypertension. *High Blood Pressure & Cardiovascular Prevention*, 2012.
[2] Lian Zenglin, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological characteristics and applications of folic acid and 5-methyltetrahydrofolate. *China Food Additives*, 2022(2).


 Online Service
Online Service
