
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






Xiao Zhou had been trying to conceive for three years, with piles of test reports for his wife.
His wife underwent hormone panel tests, ovulation monitoring, and even a hysterosalpingogram—all results were normal.
The issue lay with him.
His routine semen analysis showed no major abnormalities. A quick review by the doctor noted "average quality" and advised lifestyle adjustments: take folic acid, quit smoking, reduce alcohol intake, and exercise regularly.
Xiao Zhou followed the advice strictly. He kept folic acid by his bed and took one tablet daily without fail for over six months.
A follow-up test six months later left him stunned.
The report showed sperm concentration remained nearly identical to six months prior.
He was confused: “I took it exactly as directed—why no change? Was my folic acid intake useless?”
Later, at a reproductive center, the doctor ordered an additional MTHFR gene test. The result clarified everything: C677T, TT genotype.
This is a variant of the folate metabolism gene with extremely poor metabolic capacity. For over six months, he had taken synthetic folic acid regularly, but his body could not convert it effectively.
Xiao Zhou’s case is not unique.
Studies indicate that 78% of the Chinese population carries variations in the folate metabolism gene.
A 1,400-Participant Study Uncovers the Truth
In 2017, a study published in the Journal of Assisted Reproduction and Genetics (JARG) revealed the underlying mechanism.
Folate (vitamin B9) is critical for sperm, but with a key prerequisite.
Folate supports DNA synthesis and repair, and participates in methylation processes. Sperm production involves extremely rapid cell division with intensive DNA replication. Each division of spermatogonia relies on folate as a methyl donor to ensure stable DNA structure.
Folate deficiency reduces sperm concentration, impairs motility, increases abnormal sperm rates via elevated DNA fragmentation, lowers conception rates, and raises miscarriage risks.
The advice for men trying to conceive to take folate is valid—but the problem lies in differences between types of folate.
Normal SDF, Hidden Abnormalities in SDI
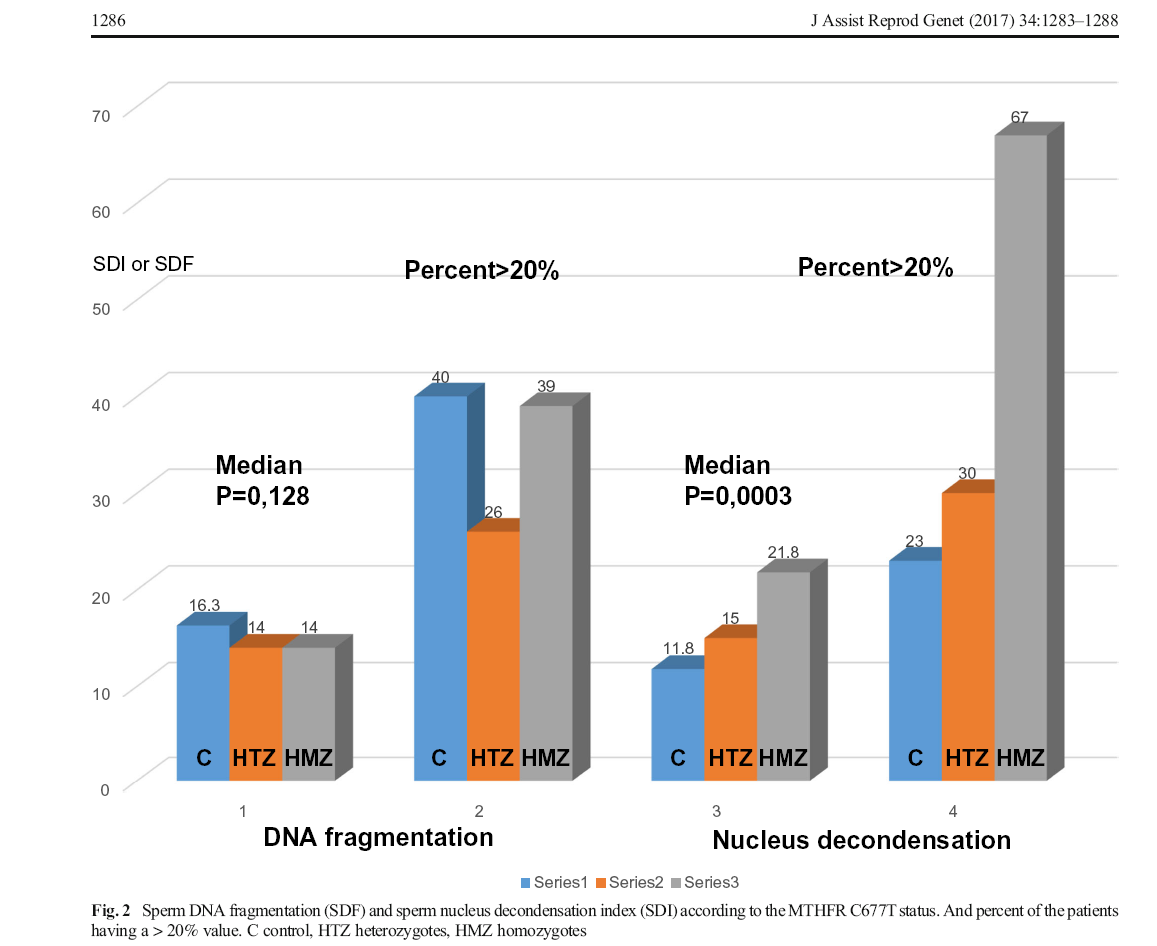
The 2017 JARG study addressed a specific question: Does the MTHFR C677T gene mutation affect sperm DNA structure?
Researchers analyzed over 1,400 infertile patients, grouping them by MTHFR genotype: normal (wild-type), CT heterozygous, and TT homozygous. They measured SDF (Sperm DNA Fragmentation) for DNA breakage and SDI (Sperm DNA Integrity) for DNA packaging compaction using flow cytometry.
Initial SDF results showed no significant differences between CT/TT carriers and the control group.
Contrary to expectations (that mutations increase DNA damage), mutation carriers had no higher sperm DNA breakage rates than normal individuals.
SDI results, however, told a different story.
TT carriers had significantly elevated SDI (p=0.0006, highly statistically significant). CT carriers also showed increased SDI (p=0.029). Using a 20% cutoff, TT carriers had a far higher rate of abnormal SDI than the control group.
The gene mutation loosens sperm DNA structure.
Broken vs. Loose DNA: The Key Difference
Sperm DNA breakage directly damages genetic material integrity, impairing embryonic development even if fertilization occurs.
Elevated SDI indicates loose DNA packaging.
During sperm maturation, DNA must be tightly folded and compacted by protamines to fit into the sperm head—a process dependent on methylation.
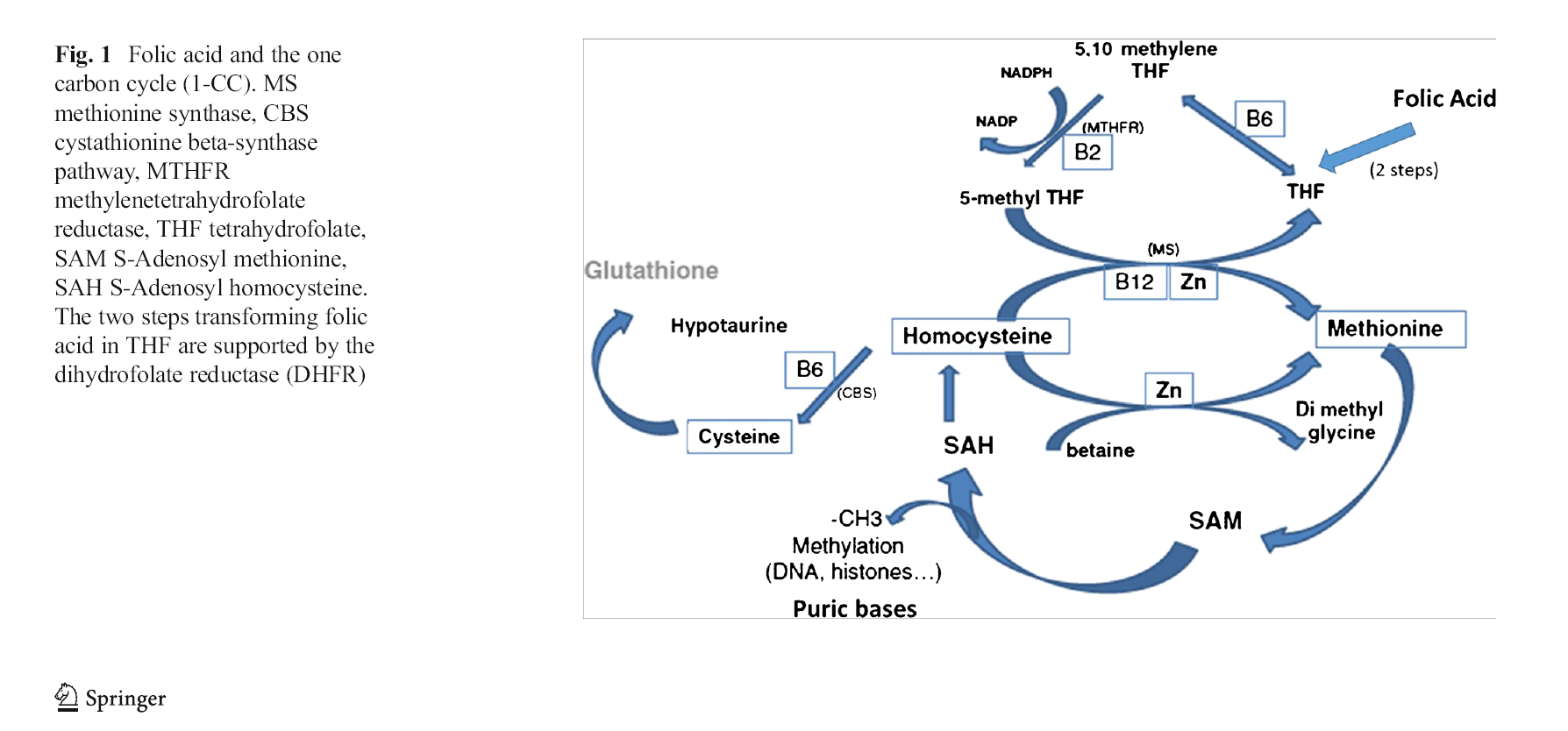
Methylation requires methyl donors, produced when the MTHFR enzyme converts folic acid into its active form: 5-methyltetrahydrofolate.
- Normal MTHFR: High enzyme efficiency, sufficient active folate, normal methylation, tight DNA packaging, normal SDI.
- Mutated MTHFR (especially TT): Severely reduced enzyme activity, insufficient active folate, impaired methylation, loose DNA structure, elevated SDI.
Elevated SDF means broken DNA strands with lost genetic information. Elevated SDI means intact genetic material but loose internal structure. During embryonic development, precise gene activation is disrupted by loose DNA, causing chaotic genome expression.
What Your Sperm Analysis Report Misses
Early or recurrent miscarriages are typically investigated in women, with tests for hormone levels, endometrial health, immunity, and chromosomes. This study highlights an overlooked factor: male MTHFR mutations can cause loose sperm DNA structure, halting early embryonic division due to gene expression errors. When female tests are normal, the cause often lies with the male.
Most reproductive centers follow WHO 5th Edition guidelines for routine semen analysis, evaluating concentration, progressive motility, and morphology. Normal results only confirm sperm quantity, mobility, and appearance—not internal DNA stability.
Routine tests ignore DNA structure. Some clinics add SDF to assess DNA fragmentation, which is an improvement. However, the JARG study confirms that MTHFR mutation carriers can have normal SDF but abnormal SDI—a hidden issue missed by SDF-only testing.
Three Critical Steps to Take
1. Genetic Testing
Xiao Zhou’s ineffective supplementation stemmed from a conversion blockage, not insufficient intake. Synthetic folic acid requires MTHFR enzyme conversion, which is drastically reduced in mutation carriers (TT carriers: <30% efficiency). Most unmetabolized folic acid never reaches sperm.
Normal routine parameters do not equal healthy sperm DNA. SDF measures breakage; SDI assesses structural compaction. Mutation carriers can have normal SDF but abnormal SDI—a key marker for unexplained infertility and miscarriage.
2. Switch to Active Folate
The solution bypasses the conversion step. The study authors recommend: Individuals with elevated SDI should undergo MTHFR genotyping and consider 5-methyltetrahydrofolate supplementation.
5-methyltetrahydrofolate (active folate) requires no MTHFR conversion and acts immediately, making it largely unaffected by genotype.
Key differences between synthetic folic acid and active folate:
- Synthetic Folic Acid: Requires MTHFR enzyme conversion; acts post-conversion; unmetabolized folic acid accumulates.
- Active Folate (5-methyltetrahydrofolate): No conversion needed; directly participates in methylation; minimal accumulation risk; mechanistically superior for improving SDI.
For mutation carriers (especially TT), choose active folate with three criteria:
1. Ingredient: 6S-5-methyltetrahydrofolate calcium (avoid products labeled only “folic acid”).
2. Dosage: Check micrograms per tablet.
3. Certification: Prioritize products with naturalization folate certification.
3. SDI Testing
After 3–6 months of supplementation, repeat routine analysis plus SDI testing. Most andrology labs offer SDI; larger reproductive centers can also perform it.
Final Notes
Folate is vital for male fertility—but for mutation carriers, the type of folate matters more than dosage.
Mutation-related sperm issues stem from loose DNA structure, caused by impaired methylation and insufficient active folate. Normal SDF does not rule out DNA problems; SDI is the critical overlooked marker.
Bypass the MTHFR bottleneck with active folate, then retest SDI to confirm restored DNA compaction.
Conception requires joint effort. After 1+ years of normal routine tests with no success, add MTHFR genotyping + SDI testing—affordable tests that may uncover the root cause of prolonged infertility.
References
[1] Journal of Assisted Reproduction and Genetics, August 2017. Association between the MTHFR-C677T isoform and structure of sperm DNA (IF=3.1). Study groups: 1,405 controls, 77 CT heterozygotes, 18 TT homozygotes. TT carriers had significantly elevated SDI (p=0.0006); CT carriers had increased SDI (p=0.029); no significant SDF differences between groups. Authors recommend MTHFR genotyping for patients with high SDI and consider 5-MTHF supplementation.
[2] Yang B, Liu Y, Li Y, et al. Geographical Distribution of MTHFR C677T, A1298C and MTRR A66G Gene Polymorphisms in China: Findings from 15,357 Adults of Han Nationality[J]. PLOS ONE, 2013, 8(3): e57917.
[3] Lian ZL, Liu K, Gu JH, et al. Biological Characteristics and Applications of Folic Acid and 5-Methyltetrahydrofolate[J]. China Food Additives, 2022(2).


 Online Service
Online Service
