
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






Sarah is 34. She has been trying to conceive for four years and has spent the last two in IVF treatment. Both embryo transfers failed.
The two embryos had already gone through strict preimplantation genetic testing. Karyotype analysis showed completely normal chromosomes. Ultrasound monitoring around ovulation showed that her endometrium had reached the expected thickness, 9 mm. Her estradiol and progesterone levels also stayed within the usual reference ranges. Routine reproductive evaluations found no obvious abnormality, and hysteroscopy showed no polyps or adhesions.
Then her reproductive specialist suggested a folate metabolism gene test.
The report read: MTHFR c.677C>T: TT genotype; c.1298A>C: AC genotype.
Sarah could not make sense of the letters and numbers. Her doctor explained that this pattern may mean her folate metabolic pathway works at only about 30% of normal efficiency. For years, she had been taking the standard 0.4 mg of regular folic acid every day.
Looking back, the problem may have been hiding at a molecular level she had never thought to check.
A 2016 study published in *Human Genetics* offers part of the explanation. Why Can a Chromosomally Normal Embryo Still Lose Its Ability to Implant?
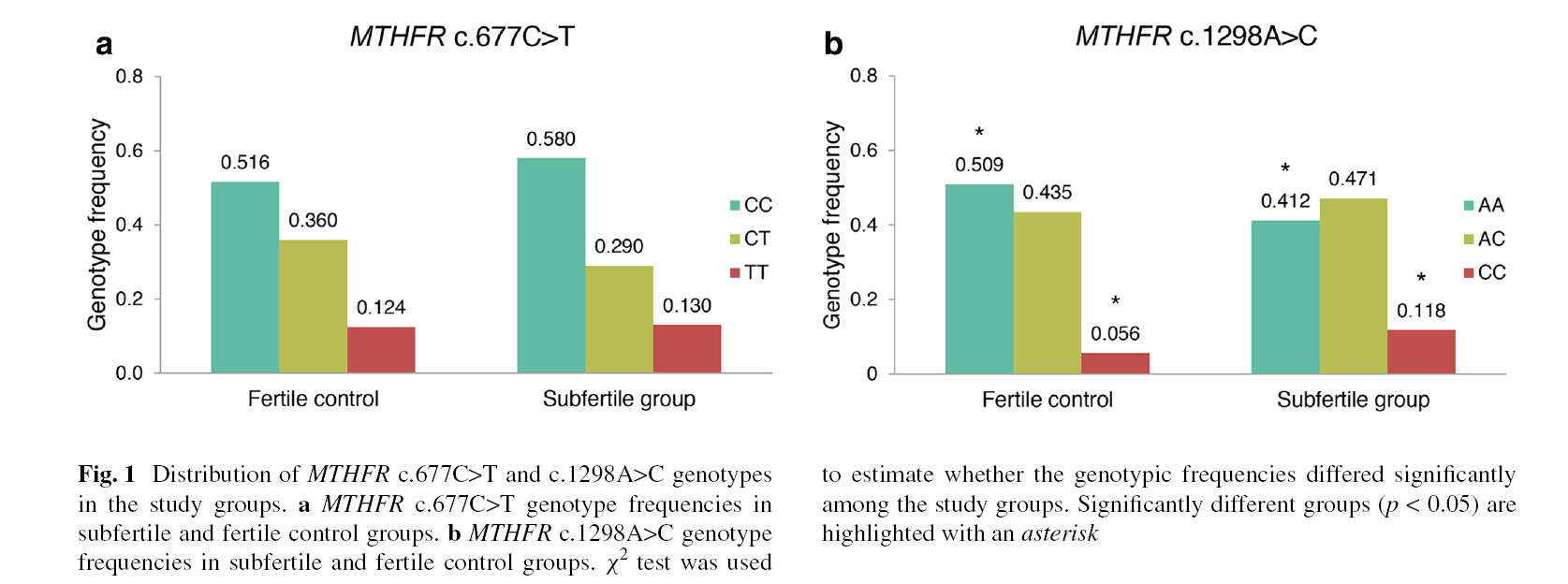
The research team focused on two common polymorphisms in the **MTHFR gene**. They recruited 138 patients undergoing assisted reproductive treatment and 161 fertile control subjects. The samples included people of European ancestry, as well as individuals with North African and Southeast Asian backgrounds. That broad ethnic mix gave the data a stronger foundation.

The findings pointed in a clear direction.
The maternal MTHFR c.1298A>C genotype significantly influenced the chance of pregnancy. The MTHFR genotypes of both parents could directly affect the formation of aneuploid embryos.
Among subfertile patients, the researchers also found an unusual pattern. In patients with a history of embryo implantation failure or miscarriage, the MTHFR c.677C>T polymorphism showed a significant deviation from Hardy-Weinberg equilibrium. In population genetics, this kind of deviation often suggests that certain genotypes are being shaped by some form of biological selection pressure within a specific group.
The more important finding centered on implantation itself.
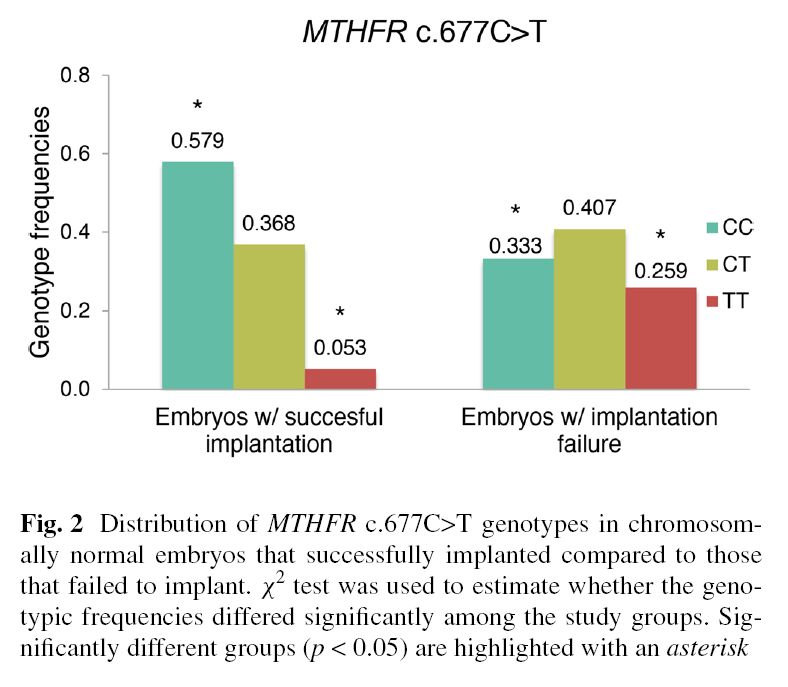
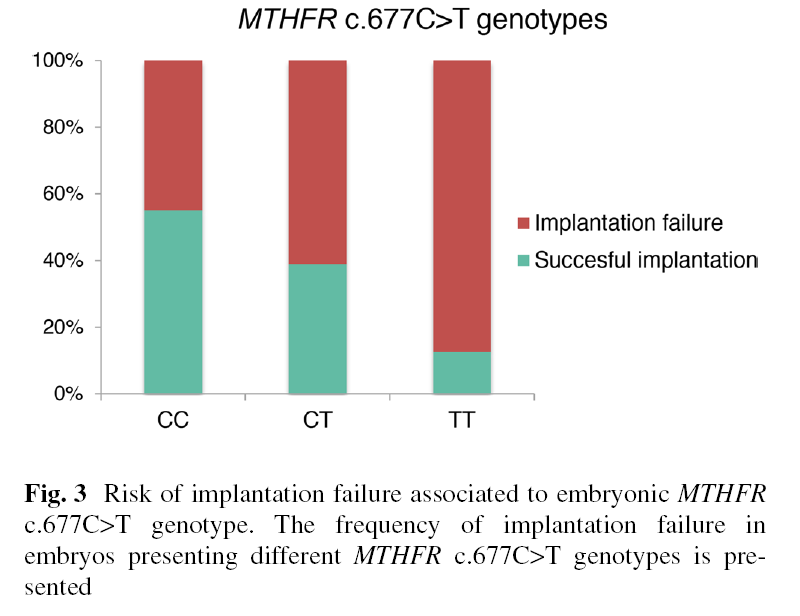
The 677T allele had a significant effect on the implantation potential of chromosomally normal embryos. That finding filled a gap clinicians had long observed.
The embryo may have the right number of chromosomes. Yet at the moment it contacts the endometrium, it may lose the biological activity needed to keep developing.
How Reduced Enzyme Activity Sets Off a Microscopic Chain Reaction
The MTHFR gene provides instructions for making methylenetetrahydrofolate reductase. This enzyme sits at the center of the folate metabolic pathway.
After folic acid enters the body, it cannot be used directly. It must go through a series of complex conversion steps. The MTHFR enzyme stands at the final, and most critical, step.
When polymorphic mutations occur, the efficiency of this step can drop sharply. In people with the c.677C>T TT genotype, MTHFR enzyme activity may be only about 30% of the normal level. If a c.1298A>C mutation is also present, the loss of enzyme activity can become even more pronounced.
Think of a factory assembly line with its most important machine running too slowly. Raw materials pile up upstream, while the finished products needed downstream remain in short supply.
Embryonic development is an intensely resource-demanding microscopic project. Rapid cell division requires large amounts of purines and pyrimidines to build new DNA. Gene expression control depends on methyl groups for DNA methylation. These processes rely heavily on the final product generated through MTHFR activity: 5-methyltetrahydrofolate.
When the supply of finished product is inadequate, flaws start to appear at the microscopic level. Chromosomes are more likely to separate incorrectly, leading to aneuploid embryos. Even when the chromosome number happens to be normal, abnormal methylation can still strip the embryo of normal physiological activity.
Transposons are like untamed horses inside the genome. Under normal conditions, methylation keeps them reined in. When methyl groups are scarce, the reins loosen. Genomic stability begins to fall apart.
Epigenetic changes are quiet. They do not alter the DNA sequence, but they can switch off key developmental genes. Once an embryo loses activity, it cannot build a stable connection with the endometrium.
Where Is the Technical Path to Bypassing the Metabolic Bottleneck?
Traditional supplementation runs into a physical bottleneck here. Regular folic acid depends entirely on MTHFR enzyme conversion. When gene polymorphisms impair enzyme activity, simply increasing folic acid intake does not solve the root problem.
It is like a major traffic jam on the main road. Sending more cars onto the same road only makes the congestion worse.
Large amounts of Unmetabolized Folic acid may accumulate in the blood. These molecules may occupy folate receptors on the cell surface, making it even harder for small amounts of active folate to be absorbed and used.
That is why directly providing the finished form has become a new direction in clinical nutrition intervention.
Supplementing 5-methyltetrahydrofolate directly can bypass the MTHFR conversion step altogether. The methyl groups and DNA synthesis materials needed for embryonic development can then be supplied in time. Choosing the right finished-form supplement, though, requires attention to several technical factors.
Stereochemical configuration is one of the key determinants of activity. The naturally occurring form is the 6S configuration of 5-methyltetrahydrofolate. Chemical synthesis can easily produce biologically inactive 6R configuration impurities. High-purity 6S extraction technology is therefore a primary screening standard.
Stability matters just as much. Free 5-methyltetrahydrofolate is highly prone to oxidation and degradation. It needs to bind with specific salts to remain active at room temperature. Calcium salt crystallization is currently a stability solution that has been validated through long-term clinical use.
Magnafolate is one option that fits these criteria. As a 6S-5-methyltetrahydrofolate calcium active folate raw material, it matches the naturally active form found in the human body in terms of spatial configuration. This raw material does not need to be converted by gene-dependent metabolic enzymes. It can cross the intestinal barrier directly into the bloodstream and take part in the microscopic work of cell division and DNA methylation.
The metabolic channel at the cellular level is opened again.
Sarah later switched to a supplement containing active folate. In her third IVF cycle, the embryo’s morphological grade was the same as before.
This time, the embryo implanted firmly.
A New Perspective on Routine Screening in Assisted Reproduction
The *Human Genetics* study established a clear link between gene polymorphisms and embryo viability. MTHFR gene testing has shown strong clinical value in assisted reproductive technology.
It is not just the reading of a single gene locus. It is a useful tool for identifying patients at higher risk of implantation failure. During IVF cycles, adjusting nutrition intervention strategies based on genetic testing may help select and culture embryos with stronger biological activity.
The shift from folic acid to active folate is, in essence, a technical adaptation to human genetic polymorphism. Clinical decision-making in reproductive medicine is moving deeper into the molecular level.
Medical progress often begins with seeing small differences clearly — and knowing when to intervene.
References
[1] Enciso M, Sarasa J, Xanthopoulou L, et al. Polymorphisms in the MTHFR gene influence embryo viability and the incidence of aneuploidy[J]. *Human Genetics*, 2016, 135(5): 555-568. doi:10.1007/s00439-016-1652-z.
[2] Yang B, Liu Y, Li Y, et al. Geographical Distribution of MTHFR C677T, A1298C and MTRR A66G Gene Polymorphisms in China: Findings from 15357 Adults of Han Nationality[J]. *PLoS ONE*, 2013, 8(3): e57917. doi:10.1371/journal.pone.0057917.
[3] Lian Zenglin, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological Characteristics and Applications of Folate and 5-Methyltetrahydrofolate. *China Food Additives*, 2022, Issue 2.
Risk Notice
Magnafolate® is supplied only as a 6S-5-methyltetrahydrofolate calcium active folate raw material. It does not provide diagnosis or treatment advice directly to consumers. Any decision about folate supplementation should be made under the guidance of a qualified physician or nutrition professional. The character in this article is a fictional case created only to help readers understand the scientific mechanism. The clinical details in the story fall within commonly seen reference ranges. Any causal interpretation in this article is strictly limited to conclusions supported by the cited literature and does not constitute a promise of product efficacy.


 Online Service
Online Service
