
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






Sarah is 29 years old. She was diagnosed with HbSS sickle cell disease more than ten years ago. Over the past year, she took folic acid tablets every day, exactly as prescribed. At her follow-up visit, her serum folate report looked good. Her doctor told her the “stores were sufficient.”
Yet in just three months, she had two acute pain episodes. In her most recent test results, several numbers stood out side by side: high-sensitivity C-reactive protein had risen to around 18 mg/L, interleukin-6 was close to 13 pg/mL, and Unmetabolized Folic acid, or UMFA, had also reached 130 ng/mL. She had not stopped supplementing. But her inflammation markers were still high.
The real question is what happens after folic acid enters the body. The folic acid residues that remain in the blood without being fully converted are now drawing more attention in clinical research.
In 2024, a study was published in the *Indian Journal of Clinical Biochemistry*. The research team focused on patients with sickle cell disease and looked at how Unmetabolized Folic acid affected immune and inflammatory markers.
They enrolled 60 diagnosed patients. Twenty-two were in an acute pain episode, while 38 were in a stable state. All of them were taking folic acid as part of their daily routine.
The researchers first measured natural killer cell activity. The data showed no clear difference between the acute episode group and the stable group.
If you only looked at that one result, it would be easy to assume that folic acid supplementation did not change immune activity. But the next set of data told a different story.
UMFA was detected in the blood of more than half of the participants. In the acute episode group, the median level reached 131.8 ng/mL. In the stable group, it was only 36.31 ng/mL.
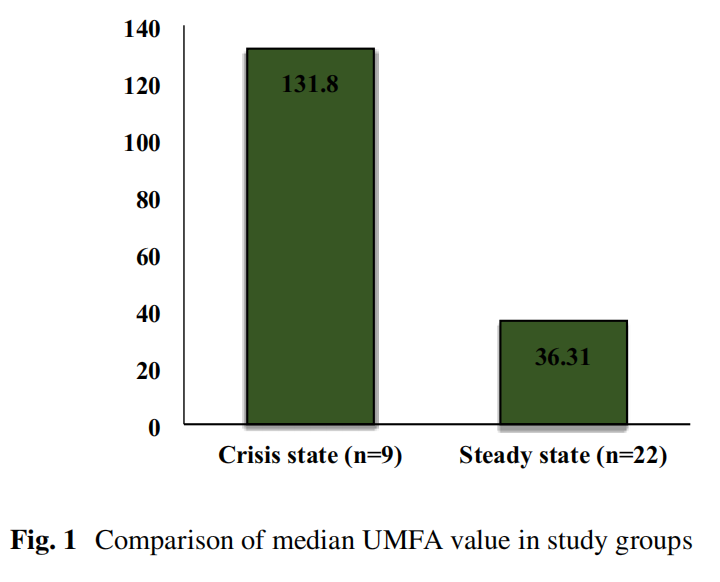
Both groups were supplementing. But patients in the acute episode phase had several times more Unmetabolized Folic acid left in their blood than those in the stable group.
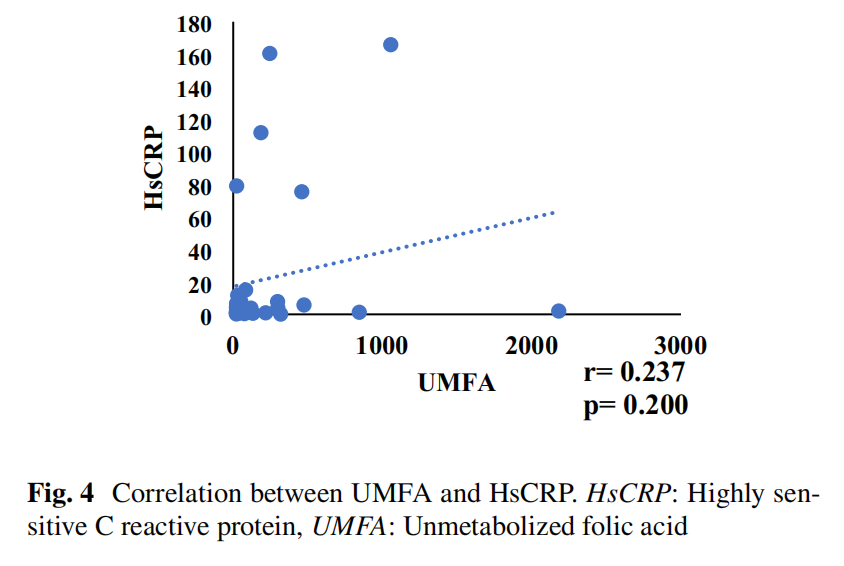
The inflammation markers also showed a wide gap. The median high-sensitivity C-reactive protein level was 18.41 mg/L in the acute episode group, compared with only 2.04 mg/L in the stable group. Interleukin-6 followed a similar pattern.
Unmetabolized Folic acid rose in step with inflammatory markers. That shifted the key question: after folic acid is supplemented, is the body actually converting and using it?
The usual thinking is that a high folate level in the blood means the body has enough nutritional reserve. But the data suggest it is not that simple.
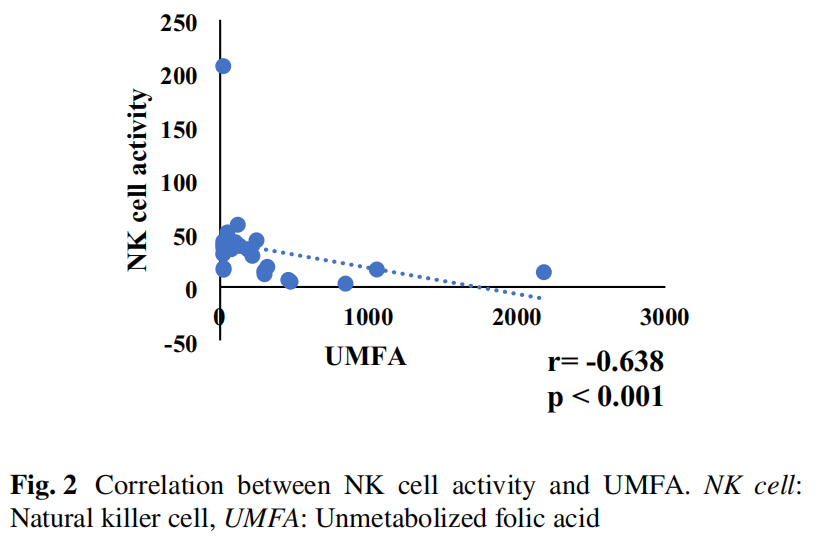
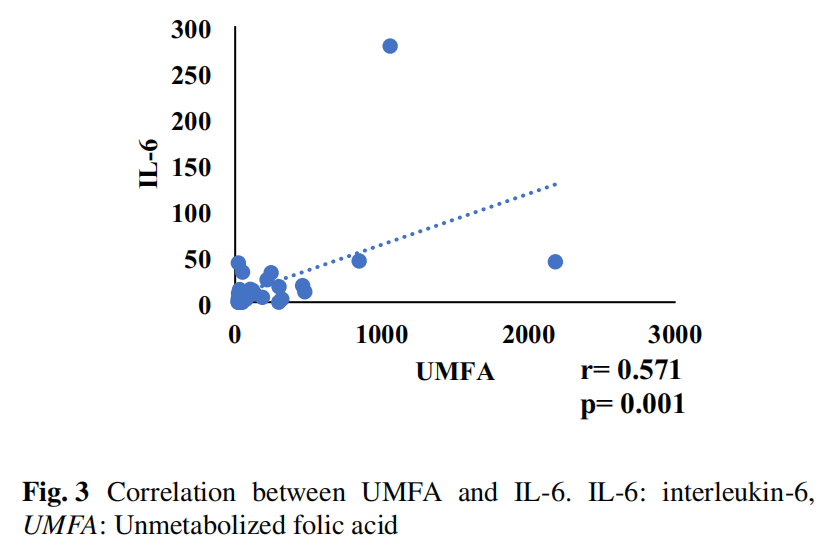
The study found that the higher the UMFA level, the lower the activity of natural killer cells. At the same time, UMFA showed a positive correlation with interleukin-6.
What does that mean?
A large amount of unmetabolized folic acid floating in the blood does not mean cells have received a usable form of folate. This buildup may interfere with normal immune cell function and may be linked to a higher risk of inflammation.
Why would this happen?
The regular synthetic folic acid people commonly take cannot be used directly by cells after it enters the body. It must go through a series of biochemical conversions and become 5-methyltetrahydrofolate, the active form that cells can recognize and use. This conversion depends on a key enzyme: 5,10-methylenetetrahydrofolate reductase, or MTHFR. But every enzyme has a processing limit. When the intake speed of folic acid exceeds the enzyme’s conversion capacity, the portion that cannot be processed in time starts to accumulate in the blood. That is how Unmetabolized Folic acid forms.
People with sickle cell disease have chronic hemolysis and a high demand for blood production, so their need for folate is already greater. But taking more does not always mean using more. If the metabolic pathway is not running smoothly, supplemented folic acid can easily get stuck during conversion. And this metabolic bottleneck is not limited to people with rare diseases.
Another study involving more than 15,000 Chinese adults found that polymorphisms in the methylenetetrahydrofolate reductase gene are widespread in the population. These genetic variants can reduce the activity of metabolic enzymes and limit conversion efficiency. For people who carry these gene variants, as well as those in special physiological stages such as pregnancy, the conversion of regular synthetic folic acid may already be less efficient.
Seen this way, the logic becomes clearer. If front-end conversion is the bottleneck, could we bypass that step and provide the body with a form that is already at the later stage of metabolism and ready to use?
The answer lies in its biochemical characteristics. 5-methyltetrahydrofolate is already downstream in the metabolic pathway, so it can bypass the limitation of 5,10-methylenetetrahydrofolate reductase, or MTHFR. Its specific active configuration, 6S-5-methyltetrahydrofolate calcium, can be used directly by the human body and has advantages in bioavailability. There are not many raw material options that meet both conditions. Magnafolate® is one of them. It is 6S-5-methyltetrahydrofolate calcium itself, so it does not need to be converted in the body and can be supplied directly for cellular use. It is positioned as an active folate raw material, not as a treatment for disease.
Still, the active form is not a cure-all.
Whether someone is ill, pregnant, or knows they carry relevant gene polymorphisms, the exact supplement dose and monitoring indicators should be determined by a qualified physician after a full evaluation. Trying to solve a complex metabolic issue simply by increasing the dose of regular synthetic folic acid may not work.
Sarah later returned for another follow-up. This time, she and her doctor did not only focus on whether she had been taking her supplements. They began looking at UMFA, 5-MTHF, and inflammation markers together. Based on her latest test results, the doctor reassessed both the form and the dose of her supplementation. Folate supplementation has never been a simple question of whether to take it or not.
How much goes in is one thing. How much the body can actually use is another. Folic acid or active folate, dosage, and each person’s own metabolic capacity all need to be considered together.
References:
[1] Effect of Unmetabolized Folic Acid on Immunoinflammatory Markers in Sickle Cell Disease Patients Taking Folic Acid Supplementation[J]. *Indian Journal of Clinical Biochemistry*, 2024 Mar.
[2] Yang B, Liu Y, Li Y, et al. Geographical Distribution of MTHFR C677T, A1298C and MTRR A66G Gene Polymorphisms in China: Findings from 15357 Adults of Han Nationality[J]. *PLoS ONE*, 2013, 8(3): e57917. doi:10.1371/journal.pone.0057917.
[3] Lian Zenglin, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological Characteristics and Applications of Folic Acid and 5-Methyltetrahydrofolate. *China Food Additives*, 2022, Issue 2.
Risk Notice: Magnafolate® is supplied only as a 6S-5-methyltetrahydrofolate calcium active folate raw material. It does not provide diagnosis or treatment advice directly to consumers. Any decision about folate supplementation should be made under the guidance of a qualified physician or nutritionist. The person described in this article is a fictional case created only to help readers understand the scientific mechanism. The detailed data in the story fall within commonly seen clinical reference ranges. Any causal interpretation in this article is strictly limited to conclusions supported by the cited literature and does not constitute a promise of efficacy for any product.


 Online Service
Online Service
