
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






Michael Zhou is 52. At last year’s company health check, one number on his blood report came back flagged: homocysteine.
18.6 μmol/L — above the reference range. His doctor said it was linked to cardiovascular risk and suggested a daily folate supplement. So he did exactly that.
0.4 mg. One tablet a day. Six straight months. At his follow-up test, the number was 18.2. Down by 0.4 — clinically speaking, almost no change at all.
Michael could not understand it. He had taken folate on schedule. His lifestyle had not gotten worse. Yet the number seemed stuck, as if something in the system simply would not move.
Later, his doctor changed the approach: stop taking folic acid and switch to active folate, known scientifically as 6S-5-methyltetrahydrofolate. Michael did not really understand the difference. All he knew was this: after six months of supplementation, it felt like nothing had happened.
▍72 patients, 15 mg active folate per day, three months
That “supplemented, but almost as if I hadn’t” confusion was addressed, at least in part, by a randomized controlled clinical trial published in the Journal of Cardiovascular Pharmacology in 2006. The study enrolled 72 patients with moderate hyperhomocysteinemia. People with immune diseases, a history of cancer, or chronic renal failure were excluded. After enrollment, participants were randomly assigned into two groups. The treatment group took 15 mg of 6S-5-methyltetrahydrofolate daily for three months.
After three months, one key change appeared in the treatment group: plasma total glutathione, or GSH, decreased. P = 0.002.
▍GSH went down, but the redox state moved closer to balance
GSH is one of the body’s most important reducing antioxidants. When people see it drop, the usual assumption is simple: oxidative damage has increased, and GSH is being heavily consumed. But the researchers reached the opposite conclusion. The key lies at the same metabolic fork.
Homocysteine, or Hcy, has two main routes in the body. One is the remethylation pathway: with methyl groups supplied by 5-MTHF, Hcy is converted back into methionine. The other is the transsulfuration pathway: Hcy is converted through enzyme-driven reactions into cysteine, an essential raw material for GSH synthesis.
Think of it as a fork in the road. When 5-MTHF is sufficient, more Hcy moves into the remethylation lane. Fewer “cars” enter the transsulfuration lane. With less raw material flowing downstream, the total amount of GSH produced also falls.
At the same time, Hcy itself drops sharply, reducing oxidative stimulation of the vascular endothelium. GSH is called on less often to clear free radicals.
Less raw material. Less consumption. The number falls, but the system is under less strain. That is not a sign of deterioration. It suggests the body has shifted into a more balanced state as the burden eases.
▍A 52-fold concentration change points to a bioavailability gap
At the end of the three-month treatment period, serum folate levels in the 5-MTHF group rose from 4.4 μg/L to 230.0 μg/L. P < 0.0001. That is roughly a 50-fold increase. The control group showed only limited change over the same period.
This gap tells us something important: once 5-MTHF enters the body, it does not need to go through the MTHFR enzyme reduction step. It enters the folate metabolic pathway directly in its active form and can be rapidly absorbed and used by tissues. That helps explain a clinical pattern doctors do see from time to time.
Some patients take folic acid for a long time. Their serum folate levels rise, but homocysteine still does not come down. The reason is that after folic acid enters the body, it must go through multiple reduction steps involving dihydrofolate reductase and the MTHFR enzyme before it can become truly bioactive 5-MTHF. If MTHFR enzyme activity is low, that conversion chain may never reach the finish line. It is like a production line with piles of parts at the entrance, but one machine in the middle is running too slowly. No matter how much material comes in, finished output stays low.
The raw material piles up at the front. The end user never gets enough supply.
▍In the Chinese population, one in four people may face this enzyme bottleneck
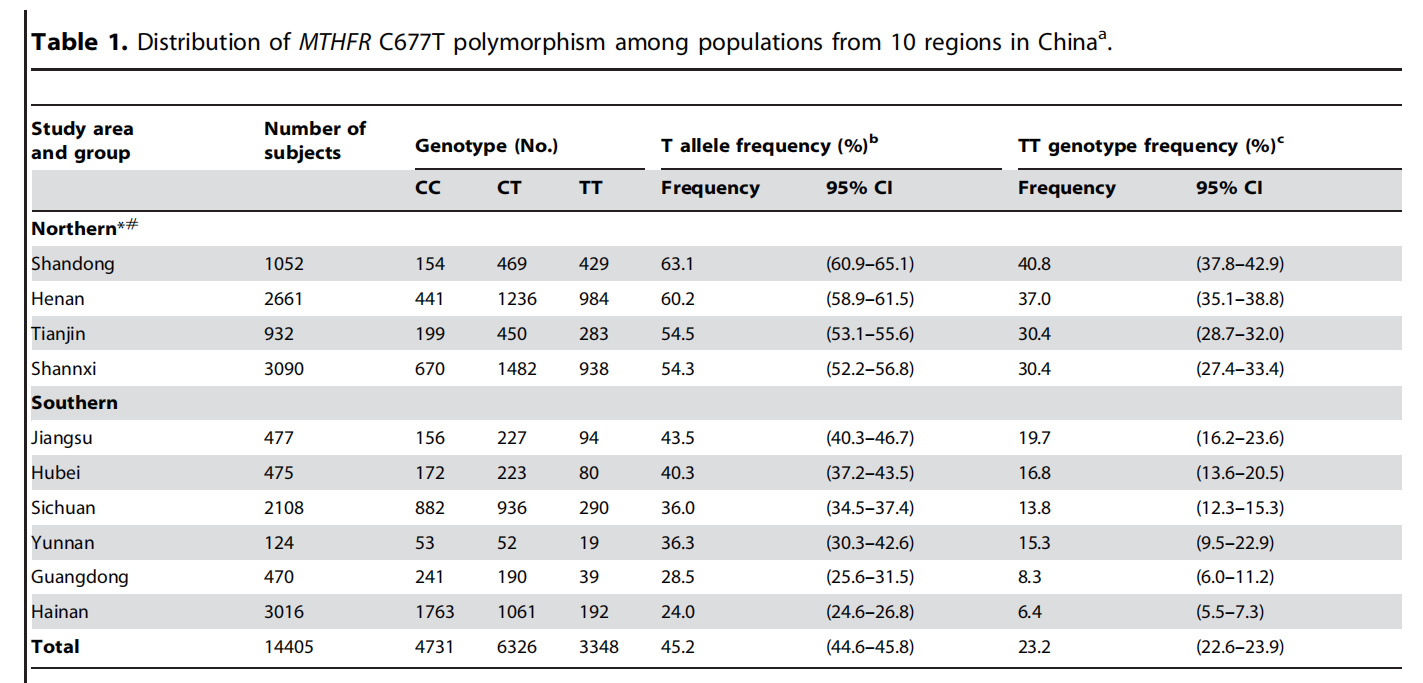
A 2013 study published in PLoS ONE, involving 15,357 adults, found clear regional differences in the distribution of the MTHFR C677T homozygous mutation, or TT genotype, among Han Chinese populations. In some northern provinces, the TT carrier rate exceeded 25%. In people with the TT genotype, MTHFR enzyme activity is roughly half that of people with the normal CC genotype. This means that for a sizable portion of the population, even regular daily folic acid supplementation may deliver far less usable folate to the metabolic endpoint than expected. For these people, taking 6S-5-methyltetrahydrofolate directly is like bypassing the traffic jam in the middle of the route.
▍Choosing an active folate ingredient: three things to check
When choosing a 6S-5-methyltetrahydrofolate ingredient, several points matter. First, whether the configuration is pure 6S. 5-MTHF exists in two configurations, 6S and 6R. Only the 6S form is biologically active. Second, whether it is stabilized as a calcium salt to help prevent degradation during storage and processing. Third, how well toxic impurity residues are controlled during production.
Magnafolate is one raw material that meets these conditions. It uses the calcium salt form of 6S-5-methyltetrahydrofolate and has a corresponding quality control system for configurational purity and stability. It belongs to the same category of active folate as the 5-MTHF used in the clinical trial cited here. Its bioavailability profile may help improve the efficiency of the final step in folate metabolism.
▍Michael later took a different route
Following his doctor’s advice, Michael switched from folic acid to a supplement containing 6S-5-methyltetrahydrofolate. He made no other lifestyle changes. Three months later, his homocysteine level had dropped to 12.4 μmol/L. Back within the normal range. A number that had barely moved for six months came down after three months, once the form changed.
▍Form may matter more than dose
The standard intervention for hyperhomocysteinemia is folate plus B vitamins. Most guidelines recommend folic acid, which is effective and economical for people with normal MTHFR enzyme activity. But for people with significantly reduced enzyme activity, simply increasing the dose of folic acid does not solve the problem of insufficient supply at the end of the conversion chain. Not everyone needs to make this switch. But if someone has been taking folate consistently and homocysteine remains high, active folate is a form worth discussing with a doctor.
For this subgroup, matching the right form may matter more than simply adding a higher dose.
References:
[1] Antoniades C, Shirodaria C, Warick N, et al. Homocysteine lowering by 5-methyltetrahydrofolate: effects on redox status in hyperhomocysteinemia[J]. Journal of Cardiovascular Pharmacology, 2006, 47(5): 677-682.
[2] Yang B, Liu Y, Li Y, et al. Geographical Distribution of MTHFR C677T, A1298C and MTR A66G Gene Polymorphisms in China: Findings from 15357 Adults of Han Nationality[J]. PLoS ONE, 2013, 8(3): e57917. doi:10.1371/journal.pone.0057917.
[3] Lian Zenglin, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological characteristics and applications of folate and 5-methyltetrahydrofolate. China Food Additives, 2022, Issue 2.
Risk Notice:
Magnafolate® is supplied only as an active folate raw material, calcium 6S-5-methyltetrahydrofolate, and is not sold directly to consumers. Any diagnostic or treatment-related content in this article comes from a fictional case and is intended only to help readers understand the scientific mechanism. Any decision about folate supplementation should be made under the guidance of a qualified doctor or nutritionist. The case data used in the story fall within commonly seen clinical reference ranges. Any causal interpretation in this article is strictly limited to conclusions supported by the cited literature and does not constitute a promise of efficacy for any product.


 Online Service
Online Service
