
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






Sarah is 52. Four years after menopause, she had a DXA bone density scan during a routine health check. Her T-scores at both the lumbar spine and femoral neck were below -2.5, and she was diagnosed with osteoporosis. She was confused. Since menopause, she had taken calcium every day without fail. Vitamin D? Covered. Vitamin K2? Also covered. Her diet was steady, and she still managed to jog three times a week. Her orthopedic doctor looked through her supplement list, then flipped through her previous biochemical test reports. He asked just one question, and it sounded odd to her: “Have you ever checked the folate level inside your red blood cells?” Sarah didn’t quite understand. As far as she knew, folate was something younger women took when preparing for pregnancy. What did it have to do with bones?
This question had already started to make sense in a 2005 study published in *Osteoporosis International*. Bone loss, as it turns out, is often more complicated than simply “not getting enough calcium.”
Why Can Bones Still Become Fragile Even When You Take Calcium?
The traditional view is that osteoporosis comes from calcium loss and falling estrogen levels. That logic is not wrong. It just leaves out another troublemaker inside the bone microenvironment. In postmenopausal women, homocysteine, or Hcy, often tends to rise. Once this metabolic byproduct builds up in the blood, it can interfere with collagen cross-linking in bone. The internal mesh-like structure of bone then becomes brittle, almost like sun-dried deadwood. To bring homocysteine down, the body needs a smooth remethylation pathway. Folate plays a key carrier role in this process, helping convert homocysteine into harmless methionine. When this pathway gets stuck, bone mineral density can quietly decline. No matter how much calcium you take, it cannot repair the underlying bone framework damaged by homocysteine.
A “Normal” Blood Folate Result May Be Misleading
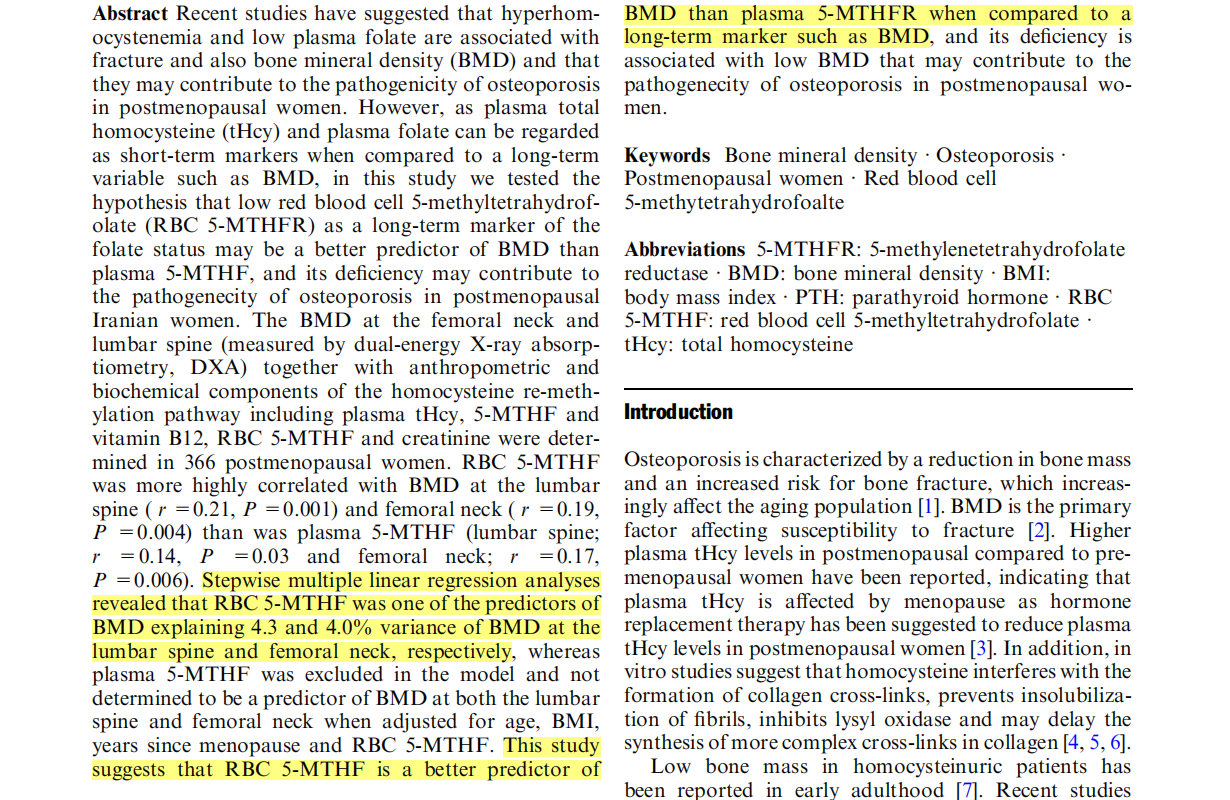
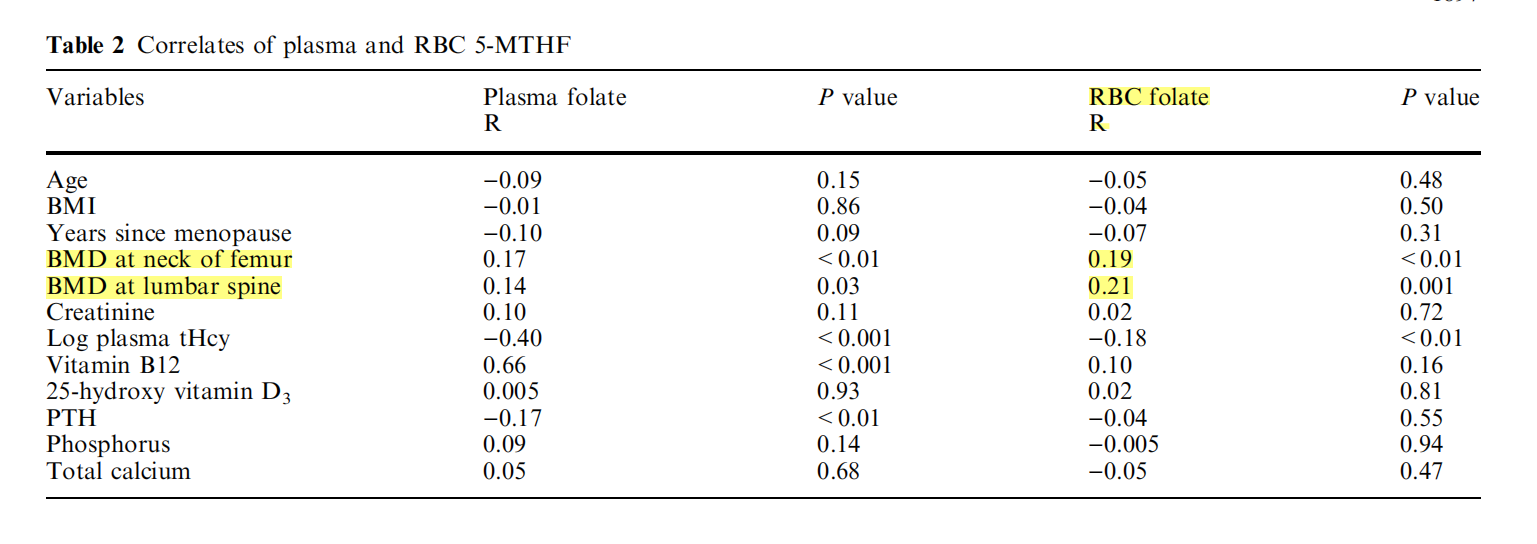
Many people have had serum folate checked during routine physical exams. The result often falls within the normal range. An Iranian research team conducted a cross-sectional analysis of 366 postmenopausal women. They measured bone mineral density at the lumbar spine and femoral neck, along with biochemical markers including serum folate and red blood cell 5-methyltetrahydrofolate, or 5-MTHF. At first glance, the surface-level data looked a little counterintuitive. When researchers looked only at serum 5-methyltetrahydrofolate, it was excluded from the multivariate linear regression model. In other words, it did not effectively predict changes in bone mineral density at the lumbar spine or femoral neck.
But another set of data told a very different story. Red blood cell 5-methyltetrahydrofolate showed a correlation coefficient of 0.21 with lumbar spine bone mineral density and 0.19 with femoral neck bone mineral density. Both were statistically significant. Multivariate linear regression showed that it was an independent predictor of bone mineral density, explaining 4.3% of the variation in lumbar spine bone mineral density and 4.0% of the variation in femoral neck bone mineral density. Serum folate is like cash in your wallet. It can rise or fall depending on what you ate over the last few meals. Red blood cell 5-methyltetrahydrofolate is more like a fixed-term bank deposit. It reflects the body’s real, longer-term reserve of active folate over the past three months. If that long-term active folate reserve is insufficient, bone mineral density loses an important support factor.
Why Regular Folic Acid May Not Be Stored in Red Blood Cells
Getting enough 5-methyltetrahydrofolate into red blood cells is not as simple as taking a few more tablets of regular folic acid. Ordinary synthetic folic acid, or FA, has no biological activity on its own after entering the body. It must go through multiple steps of metabolic reduction in the liver and intestines, with the help of the MTHFR enzyme, before it can finally become 5-methyltetrahydrofolate and participate in homocysteine breakdown. And that conversion step is exactly where many people run into trouble.
Among the Han Chinese population, the carrier rate of the MTHFR C677T gene polymorphism is very high. The TT homozygous mutation genotype is found in about 25% of people. In those who carry this variation, the activity of the conversion enzyme drops significantly. The folic acid they take cannot be efficiently converted. Instead, it may circulate in the blood as Unmetabolized Folic acid, or UMFA. It does not effectively enter red blood cells, and it cannot help clear homocysteine around bone tissue. Middle-aged and older adults already tend to absorb nutrients less efficiently. Add a genetic metabolic barrier on top of that, and the body’s internal defense line for bone health can start to weaken from within.
A More Targeted Way to Bypass the Conversion Bottleneck
If the conversion enzyme is not reliable, then directly supplementing active folate that does not require metabolic conversion becomes a practical way around the bottleneck. Structurally, active folate is 6S-5-methyltetrahydrofolate. It does not need MTHFR enzyme catalysis. The body can absorb and use it directly, allowing it to enter red blood cell reserves more quickly while helping lower homocysteine levels in the blood more efficiently. When choosing an active folate ingredient, stability and safety matter most. Traditional active folate can oxidize and lose potency when exposed to air, temperature changes, or humidity. Raw materials improved through crystalline technology can better maintain high activity during long-term storage and after entering the body. There are not many raw materials today that can achieve high crystalline stability. Magnafolate is one of them. This patented C-crystal form of 6S-5-methyltetrahydrofolate calcium has a longer mean residence time in terms of bioavailability, helping maintain a steadier effective concentration in the blood. It carries no risk of Unmetabolized Folic acid accumulation and does not mask vitamin B12 deficiency symptoms, which are relatively common in middle-aged and older adults. That makes it a suitable option for long-term nutritional supplementation.
Following her doctor’s advice, Sarah later adjusted her daily supplement plan. She replaced her regular B-complex vitamin with a formula that directly contained active 5-methyltetrahydrofolate. At her follow-up check six months later, her homocysteine level had dropped into the safe range. Bone aging is a long and complex process. Calcium and vitamin D intake still matter, of course. But keeping the body’s one-carbon metabolism running smoothly, and controlling the erosion of the bone matrix by homocysteine, is also an important part of protecting bone mineral density.
References
[1] Razavi M, Jafari M, et al. Association of red blood cell 5-methyltetrahydrofolate folate with bone mineral density in postmenopausal Iranian women[J]. *Osteoporosis International*, 2005, 16(12): 1884-1889.
[2] Yang B, Liu Y, Li Y, et al. Geographical Distribution of MTHFR C677T, A1298C and MTRR A66G Gene Polymorphisms in China: Findings from 15357 Adults of Han Nationality[J]. *PLoS ONE*, 2013, 8(3): e57917. doi:10.1371/journal.pone.0057917.
[3] Lian Zenglin, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological characteristics and applications of folic acid and 5-methyltetrahydrofolate. *China Food Additives*, 2022, Issue 2.
Risk Notice
Magnafolate® is supplied only as an active folate raw material of 6S-5-methyltetrahydrofolate calcium. It is not intended to provide diagnosis or treatment advice directly to consumers. Any decision about folate supplementation should be made under the guidance of a qualified physician or nutritionist. The character in this article is fictional and is used only to help readers understand the scientific mechanism. The details and data in the story fall within commonly seen clinical reference ranges. Any causal interpretation in this article is strictly limited to conclusions supported by the cited literature and does not constitute a promise of efficacy for any product.


 Online Service
Online Service
