
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






Michael is 58 this year. For years, his physical exam reports showed blood pressure and lipid numbers that were not bad at all. But over the past six months, he began to feel tightness in his chest after climbing to the third floor. A few minutes of rest would ease it. He later had coronary angiography. The result: three-vessel disease. Then came the familiar numbers again: blood pressure 135/85 mmHg, LDL cholesterol 2.1 mmol/L, homocysteine 11.5 μmol/L. All within clinically acceptable ranges. Routine tests did not point to one obvious trigger. Later, his doctor added a red blood cell folate test and followed up with genetic screening. That was when Michael began to understand something: his coronary artery problem might be linked to a nutrient he had always assumed was “covered” as long as he took enough of it.
This case points to an often-overlooked marker in routine cardiovascular risk assessment — one that may carry real decision-making value.
▍ Even when routine markers look fine, hidden vascular risks may still be there
In 2005, *Heart and Vessels* published a cross-sectional study from Shiraz, southern Iran [1].
The study included 251 patients under 70 years old with angiographically confirmed coronary artery disease. They were grouped by the extent of coronary involvement: single-vessel, double-vessel, or three-vessel disease. Researchers recorded plasma total homocysteine, MTHFR C677T genotype, and red blood cell 5-methyltetrahydrofolate (5-MTHF) concentration. One point matters here. Plasma folate is easily affected by recent diet. Red blood cells live for about 120 days, so red blood cell 5-MTHF better reflects longer-term folate reserves over the past few months. The finding was straightforward: as the number of affected coronary vessels increased, red blood cell 5-MTHF concentrations dropped significantly (ANOVA, P<0.001).
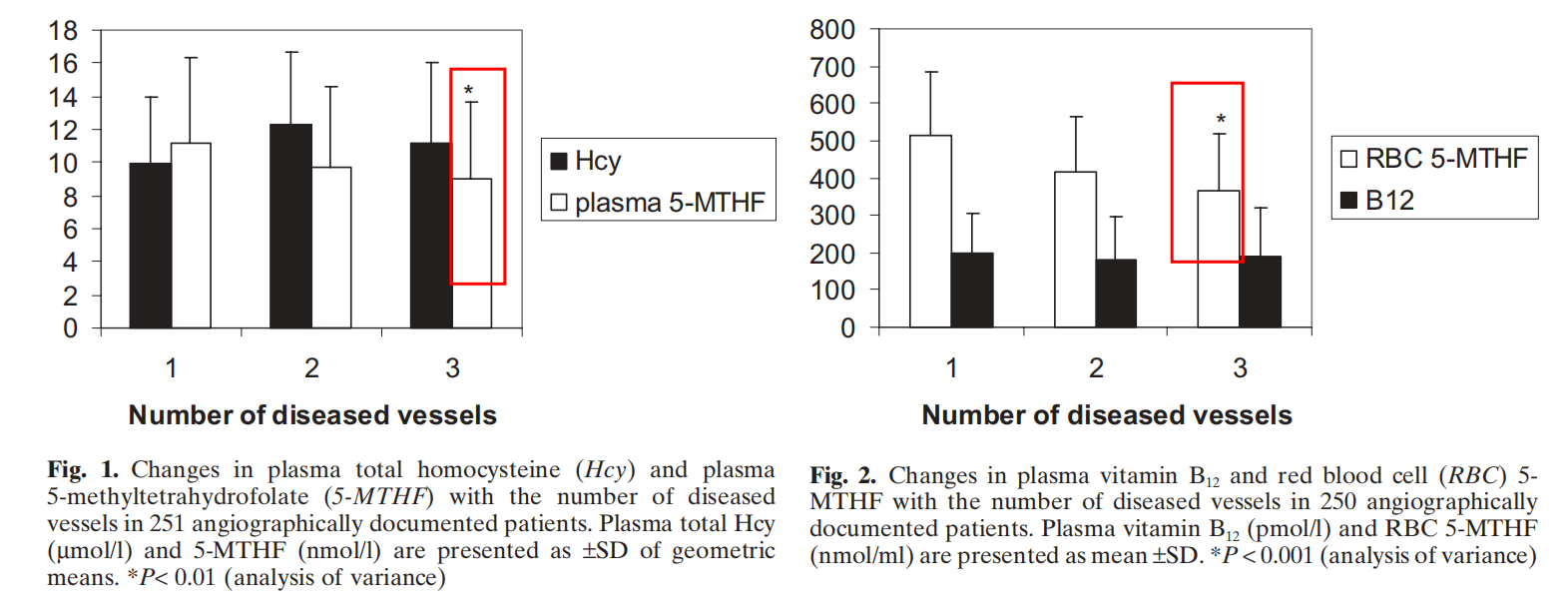
The regression analysis added more detail. After homocysteine, MTHFR C677T genotype, and other coronary artery disease risk factors were included in the model, red blood cell 5-MTHF remained independently associated with disease extent (beta = −0.002, P<0.001, model r² = 0.128). The study also reported a negative correlation between the two variables (reported r≈−0.36, P<0.001). In the conventional view, the link between folate and cardiovascular health is often explained through homocysteine. Elevated Hcy can promote oxidative stress, damage the vascular endothelium, and increase the risk of atherosclerosis. But this dataset suggests something else: even when homocysteine is not elevated, inadequate long-term active folate reserves may still be associated with a wider extent of coronary involvement — independent of Hcy level, MTHFR genotype, and routine risk factors. Not every risk shows up on a lipid panel.
▍ Red blood cell 5-MTHF: the blood vessels’ long-term reserve
5-MTHF is the active form through which folate participates in one-carbon metabolism. It helps remethylate homocysteine into methionine and is involved in the generation of methyl donors such as S-adenosylmethionine. The vascular wall is dealing with more than cholesterol deposition. Oxidative stress, chronic inflammation, and fluctuations in endothelial function can all contribute to plaque formation and narrowing. Animal and cell studies offer some clues. Calcium 6S-5-methyltetrahydrofolate has been shown in cerebral ischemic injury models to increase the activity of glutathione peroxidase and superoxide dismutase, while lowering malondialdehyde levels [2]. In inflammatory models, it reduced the recruitment of neutrophils and macrophages to inflammatory sites and decreased the release of pro-inflammatory factors such as IL-6, IL-1β, and TNF-α. Some clinical observations also found that patients receiving 5-MTHF intervention had lower C-reactive protein levels than those taking regular folic acid at 24- and 55-month follow-up. These findings should not be simply extrapolated into claims about the effects of any specific product. Still, they help explain one phenomenon: red blood cell 5-MTHF is not just an isolated nutrition number. It is more like a metabolic reserve that blood vessels draw on while facing long-term oxidative and inflammatory pressure. When that reserve is low, the system is more likely to come under strain.
▍ Why active folate may still be low even after taking regular folic acid
Regular folic acid cannot be used by cells immediately after it enters the body. It has to go through several steps of reduction and methylation before it is finally converted into 5-MTHF and enters one-carbon metabolism. In other words, regular folic acid must be converted before it becomes 5-MTHF, and the MTHFR enzyme is responsible for part of that conversion process.
In 2013, Yang B and colleagues analyzed more than 15,000 Han Chinese adults [2]. They found that folate-metabolism-related genetic polymorphisms — including MTHFR C677T, A1298C, and MTRR A66G — are widely distributed in the population. In some regions, the proportion of people with the C677T TT homozygous genotype reached about one quarter. When MTHFR enzyme activity is affected by genetic polymorphisms, the efficiency of converting regular folic acid into 5-MTHF may be limited. That is when a gap can appear: someone is taking folic acid, but their red blood cell active folate reserve does not rise accordingly. Unmetabolized Folic acid is another factor to watch. When regular folic acid intake is high, or when conversion capacity is limited, Unmetabolized Folic acid may accumulate in the blood. Related animal studies suggest that high-dose synthetic folic acid may be associated with adverse cardiovascular development-related findings in certain models. Middle-aged and older adults also often face a risk of vitamin B12 insufficiency, so assessing B12 status matters in real life when regular folic acid is taken in large amounts over the long term. The problem may not be whether folate was taken. It may be whether the body can convert it smoothly after intake.
▍ How to think about active folate: three dimensions to consider
For people with persistently low red blood cell folate, possible MTHFR metabolic bottlenecks, or elevated homocysteine, several factors are worth reviewing together. Serum folate is easily influenced by recent diet. Red blood cell folate is better for observing folate status over a period of time, so it can be used to assess longer-term reserves first. MTHFR genotype, homocysteine, vitamin B12, and vitamin B6 are best interpreted together. The broader metabolic background matters.
Regular folic acid needs conversion. 5-MTHF is the active form and can bypass part of the limitation related to MTHFR. For people whose conversion efficiency is uncertain, active folate is an option worth discussing. When looking at the ingredient itself, stability, impurity control, and in-body release characteristics all deserve attention. 5-MTHF is relatively reactive. If its stability during processing and storage is insufficient, the retained activity at the time of actual intake may be affected. Take the C-crystal form of calcium 6S-5-methyltetrahydrofolate as an example. Existing research shows that the C-crystal form can remain stable for more than 48 months at room temperature. Pharmacokinetic studies suggest an average residence time of about 3.7 hours, indicating a relatively longer stay in the body and steadier release [3]. In terms of impurity control, the 5-MTHF oxidation product JK12A has shown dose-related adverse effects in zebrafish embryo models. Studies on the C-crystal form have evaluated and discussed the safety and control of such impurities. Magnafolate, the C-crystal form of calcium 6S-5-methyltetrahydrofolate, is one example of this type of ingredient. This discussion is about ingredient quality standards. It should not be read as a promise of any clinical outcome.
▍ A cardiovascular metabolism checklist
Michael later continued standard treatment under the care of his cardiologist. His doctor reviewed his red blood cell folate, homocysteine, vitamin B12, and genetic results together, then adjusted his nutrition plan. A few months later, his red blood cell folate had returned to the follow-up target range. Michael’s story is only here to help explain the mechanism. It should not be treated as causal evidence. What is truly useful is this checklist:
When assessing vascular risk, do not look only at blood pressure, blood lipids, and blood glucose. For people who already have coronary artery disease, a strong family history, elevated homocysteine, or long-term folate supplementation with unsatisfactory markers, it may help to ask four more questions during review:
• Is red blood cell folate sufficient?
• Is there an MTHFR metabolic bottleneck?
• Is vitamin B12 on the low side?
• Should the supplement form shift from “raw material” to “active form”?
Put simply, it means looking at metabolism from a more complete angle. Regular folic acid is like raw material. Active folate is like a finished product that has already gone through the key processing steps. Some people’s metabolic assembly line just does not run efficiently. Providing the finished form directly can be one way to support nutrition while bypassing the bottleneck.
References
[1] Sadeghian S, Fallahi F, Salarifar M, et al. Association of red blood cell 5-methyltetrahydrofolate and severity of coronary artery disease: a cross-sectional study from Shiraz, southern Iran[J]. *Heart and Vessels*, 2005, 20(5): 202–207.
[2] Yang B, Liu Y, Li Y, et al. Geographical Distribution of MTHFR C677T, A1298C and MTRR A66G Gene Polymorphisms in China: Findings from 15357 Adults of Han Nationality[J]. *PLoS ONE*, 2013, 8(3): e57917. doi:10.1371/journal.pone.0057917.
[3] Sarah Lian, Michael Liu, Grace Gu, David Cheng, et al. Biological characteristics and applications of folic acid and 5-methyltetrahydrofolate. *China Food Additives*, 2022(2).
Risk Notice
Magnafolate® is supplied only as an active folate ingredient, calcium 6S-5-methyltetrahydrofolate. It is not intended to provide diagnosis or treatment advice directly to consumers. Any decision about folate supplementation should be made under the guidance of a qualified physician or nutrition professional. The person in this article is a fictional case used only to help readers understand the scientific mechanism. The detailed data in the story fall within commonly seen clinical reference ranges. Any causal interpretation in this article is strictly limited to conclusions already supported by the cited literature and does not constitute a promise of efficacy for any product.


 Online Service
Online Service
