
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






“BP 140/90, homocysteine 19.2 µmol/L.” At 32 weeks, Emily crumpled the prenatal report in her hand. “I take folic acid religiously—how did this happen?”

An MTHFR gene test gave her the answer: C677T genotype TT—a variant she had never heard of, yet the missing piece of her puzzle.
A 2021 paper in the American Journal of Translational Research mapped out exactly how MTHFR 677TT tips the scale toward gestational hypertension (GH).
Researchers paired 180 GH patients with 180 normotensive controls and spotted two glaring differences:
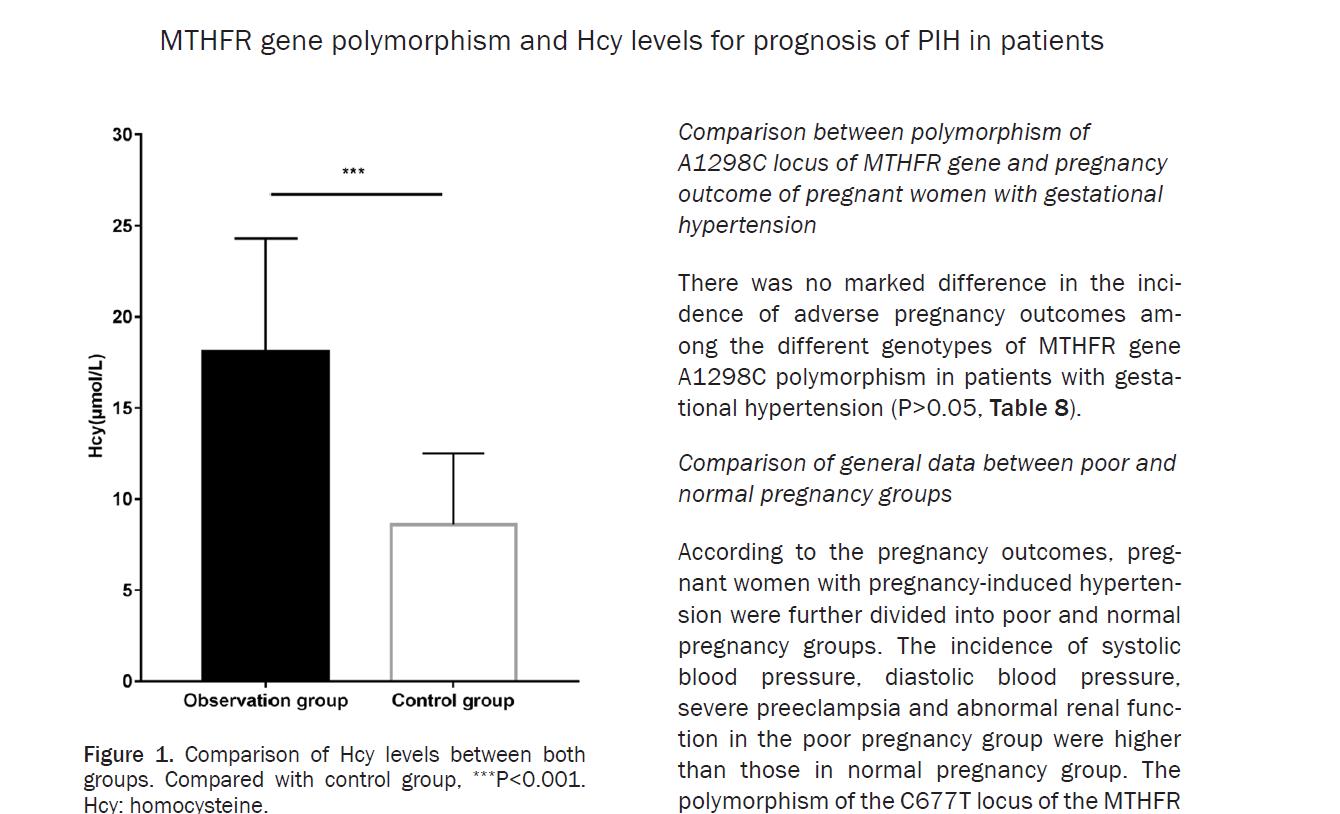
1. Hcy gap. Mean homocysteine in GH mothers was 18.1 ± 6.2 µmol/L—more than double the 8.6 ± 3.9 µmol/L seen in controls (p < 0.001). Hcy is the metabolic stop-gap when folate processing stalls; the higher it climbs, the steeper the risk for GH, placental abruption and growth restriction.
2. Gene gap. The “fast” CC genotype was under-represented in GH cases, while the “slow” CT and TT types were over-represented (p < 0.001). TT mothers posted the highest Hcy values and the worst perinatal outcomes—preterm delivery, fetal distress—far above CC or CT peers (p < 0.01).

Bottom line: if you carry CT or TT at MTHFR C677T, your ability to convert synthetic folic acid into usable 5-methyltetrahydrofolate is blunted. You can swallow the recommended 400 µg daily and still watch Hcy—and your blood pressure—rise. That is exactly what happened to Emily.
Naturalization Folate: a straight-through lane for “slow” metabolizers
If folic acid demands conversion, is there a form that bypasses the enzyme
bottleneck?
Yes—6S-5-methyltetrahydrofolate calcium, the body’s end-active folate. It requires no MTHFR step; it is absorbed as-is.

Magnafolate—the patented, C-crystalline form of this active folate—was developed without formaldehyde or p-toluenesulfonic acid. Toxic impurities such as JK12A and 5-Methyltetrahydropteroic acid are driven below detection limits, earning an “essentially non-toxic” rating from Shanghai CDC—reassuring for the most vulnerable populations.
Clinical data show Magnafolate raises serum and red-cell folate faster than folic acid, shaving Hcy down to target within weeks.

So if your prenatal screen flags high Hcy, erratic BP or an MTHFR variant, relax—your body is simply asking for a smarter folate. Discuss with your provider whether switching from folic acid to Magnafolate is right for you.
Every expectant mother wants an uneventful pregnancy. Choosing the correct folate source is the first, smallest, yet most decisive step.
Disclaimer
Magnafolate® is a bulk ingredient (6S-5-methyltetrahydrofolate calcium); it is
not a drug and is not sold directly to consumers. Any supplementation change
requires professional medical supervision.
Case story dramatized from pooled research data, not an individual patient record.
Reference:
[1] Zhang LJ, Sun LL, Wei T. Correlation between MTHFR gene polymorphism and homocysteine levels for prognosis in patients with pregnancy-induced hypertension. Am J Transl Res. 2021 Jul 15;13 (7):8253-8261. eCollection 2021. PMID: 34377314; PMCID: PMC8340186.


 Online Service
Online Service
