
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 






Since becoming a mother, the word “nutrition” has taken root in my heart, carrying a weight I never felt before. From the moment I conceived to the breastfeeding period, I have made folate a daily must‑do without fail. But have you ever stopped to ask: Is all the folate we take effectively converted in the body into nutrition our baby can actually absorb?
1. A Wake‑Up Call from Research: High‑Dose Folic Acid May Lead to Accumulation of Unmetabolized Folic Acid
In 2018, The Journal of Nutrition published a Canadian study that raised important concerns.
The study enrolled 117 healthy lactating women. From mid‑pregnancy onward, they took 1000 μg of folic acid plus 12 μg of vitamin B₁₂ daily, continuing until 8 weeks after delivery. Blood samples collected at 8 weeks postpartum were analyzed for folate forms.
Findings revealed a more serious situation than expected: Unmetabolized Folic Acid was detected in 93% of samples, with a median concentration of 2.21 nmol/L and a maximum of 144 nmol/L — figures that demand attention.
More critically, the researchers identified a threshold: when serum total folate did not exceed 78.5 nmol/L, there was no clear link between unmetabolized folic acid and total folate. However, once this threshold was crossed, each 1 nmol/L increase in total folate was accompanied by a 0.78 nmol/L rise in unmetabolized folic acid (P<0.001), showing strong correlation.
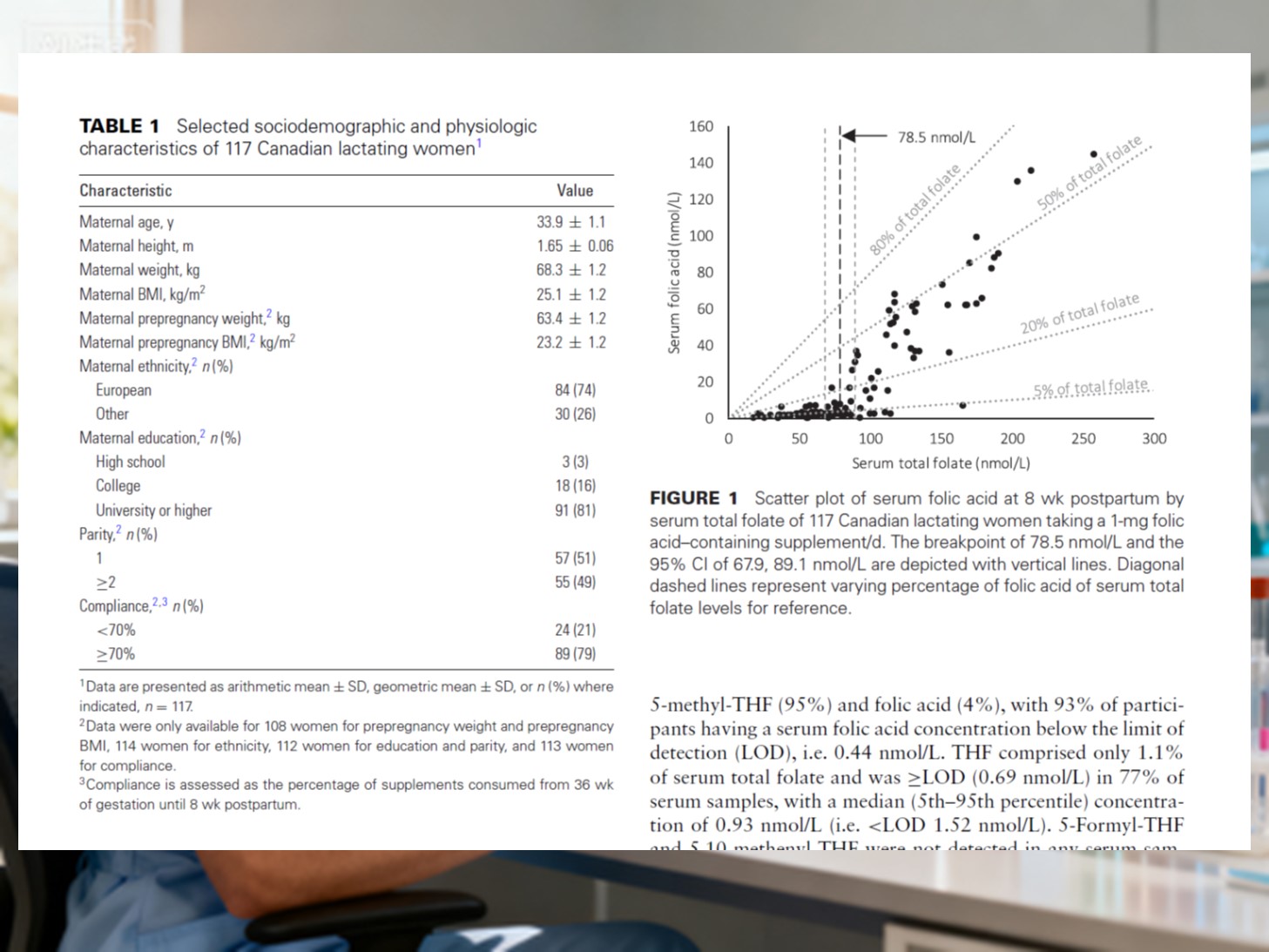
As folate intake rose, the proportion of unmetabolized folic acid within total folate surged from 2% in the lowest group to 41% in the highest — an increase of more than twentyfold.
Interestingly, the team ruled out oxidation or degradation products as the cause, because concentrations of such metabolites (MeFox) did not differ across groups. In other words, what accumulated was unaltered folic acid that had not been converted, simply remaining in circulation.
The study’s conclusion is straightforward: long‑term daily supplementation of 1000 μg folic acid may result in nearly half of lactating women having “unused and unexcretable” unmetabolized folic acid quietly suspended in their bloodstream.
2. Why Does This Happen? The Metabolic “Bottleneck” of Folic Acid
Dietary folate cannot be used directly by our bodies.
It must first undergo enzymatic processing in the liver (via enzymes such as dihydrofolate reductase) to become the main active form in blood — 6S‑5‑Methyltetrahydropteroic acid (Naturalization folate) — before cells can utilize it.
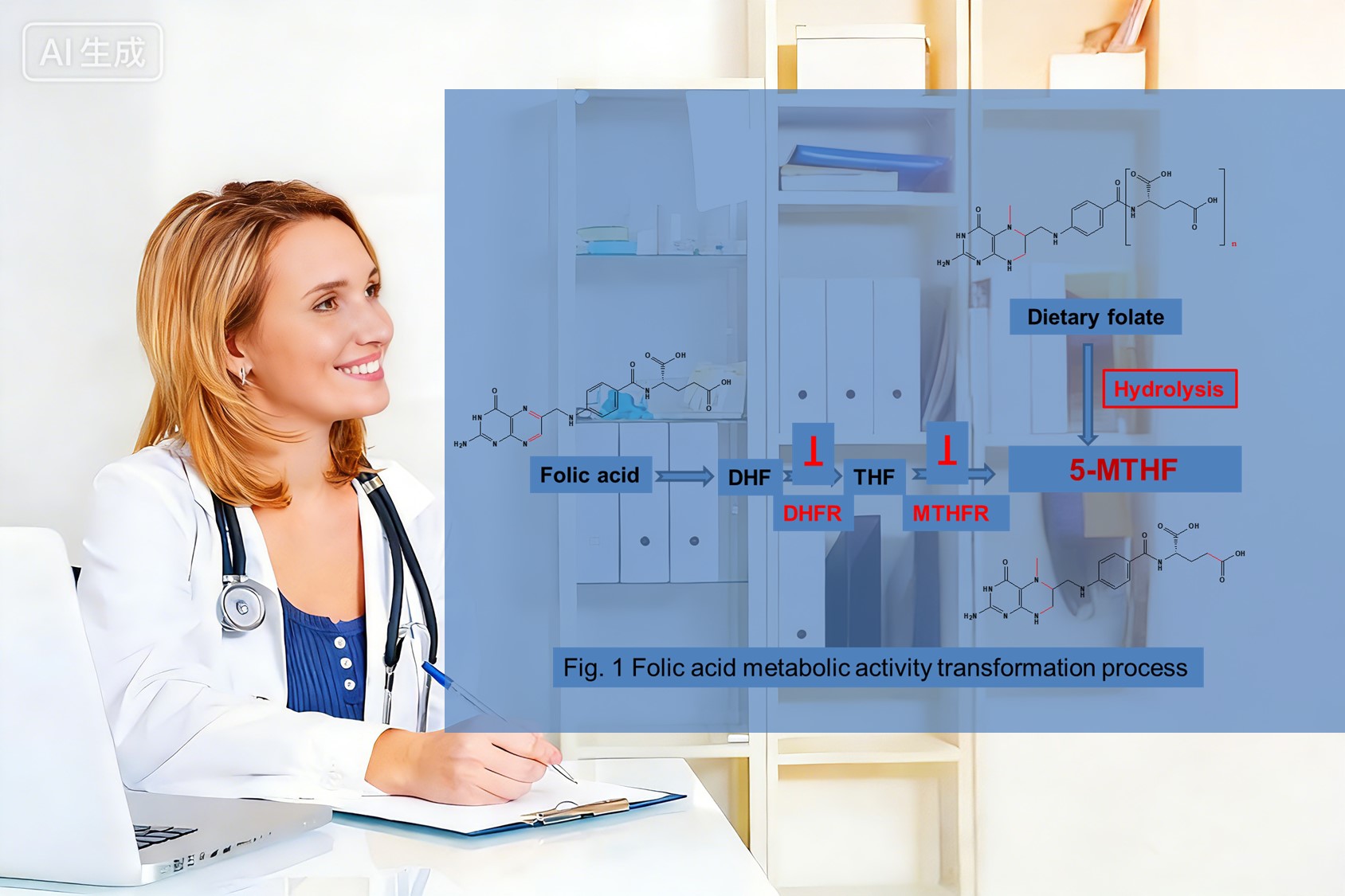
However, this conversion process resembles a production line with limited speed and capacity. If too much synthetic folic acid is ingested too quickly, the liver may become overloaded; some folic acid will remain unconverted and circulate in its original form — this is unmetabolized folic acid.
Studies suggest that unconverted folic acid is not merely idle — it may interfere with the interpretation of folate metabolism markers and potentially affect immune function. Hence, the Canadian study recommended reconsidering folate dosage during pregnancy and lactation, and proposed providing folate already in its active form to bypass hepatic conversion, thereby reducing risks linked to unmetabolized folic acid accumulation.
3. A Safer Choice: Magnafolate® — Naturalization Folate
Faced with these findings, many mothers understandably worry: “How can I supplement safely?”
The answer may lie in active folate — particularly Magnafolate, which has passed safety testing by Shanghai CDC and is classified as practically non‑toxic.

Unlike folic acid, which requires hepatic conversion, Magnafolate is already in the body‑ready active form. It can be absorbed directly and enter circulation swiftly, avoiding “traffic jams” in metabolism that leave unmetabolized residues. It is also unaffected by metabolic variations such as MTHFR gene polymorphisms, meaning individuals with low enzyme activity still receive adequate usable folate. Most importantly, it does not produce the unmetabolized folic acid buildup observed in studies, thereby reducing potential excess risk at the source.
Research indicates that future folate strategies might prioritize direct provision of active folate to ease unnecessary metabolic burden and unknown risks.
4. Our Shared Hope: Enough, and the Right Kind
Every parent wants to give their child the best nutrition.
I truly understand that feeling — wanting to provide plenty, yet fearing overdoing it.
Today, with scientific progress, we are moving beyond the simplistic notion of “more is better.” We are paying closer attention to folate’s form, whether it can be directly absorbed, and the risks of unmetabolized folic acid accumulation — making it possible for folate to reach the baby’s body more effectively and safely.

Therefore, a folate such as Magnafolate®, which is already in active form and ready for direct use, can ensure every act of care reaches exactly where the baby needs it most.
Note: Choose the type and dose of folate under the guidance of a physician or dietitian.
References
[1] Lamers Y, Prinz-Langenohl R, Braam L A, et al. Lactating Canadian Women
Consuming 1000 μg Folic Acid Daily Have High Circulating Serum Folic Acid Above a
Threshold Concentration of Serum Total Folate. The Journal of Nutrition, 2018, 148(8):
1252–1259. DOI: 10.1093/jn/nxy070.
[2] Lian Z, Liu K, Gu J, Cheng Y. Biological Characteristics and Applications
of Folate and 5‑Methyltetrahydropteroic Acid. China Food Additives, 2022(2): 229–238.


 Online Service
Online Service
